![]()
1
Anatomy of the Heart for a Dissector
Farhood Saremi1 & Damián Sánchez-Quintana2
1University of California Irvine, CA, USA
2University of Extremadura, Badajoz, Spain
Introduction
This chapter provides a general description of the heart anatomy and offers an outline of the relevant clinical information. Images are produced using state of the art multidetector scanner on living subjects and by meticulous dissection techniques on cadaveric specimens. Detailed discussions on specific anatomic locations are presented in the subsequent chapters.
Heart Orientation within the Thorax
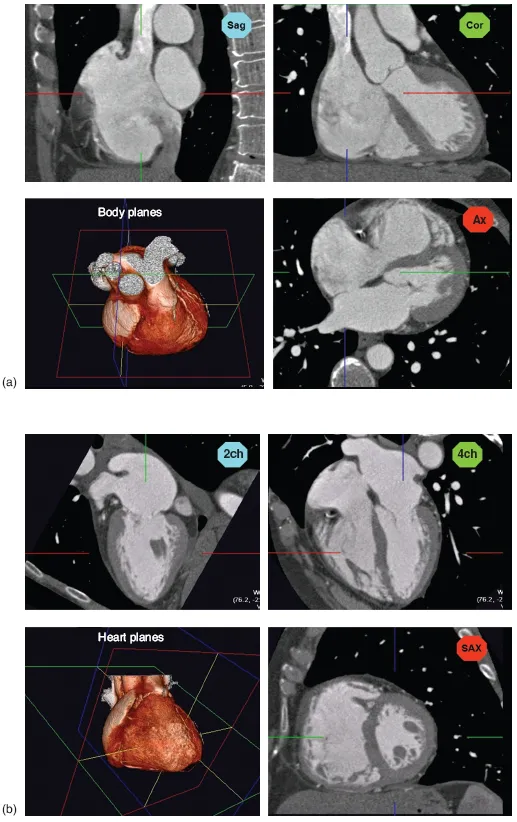
Generally, cross-sectional imaging study of the heart requires reconstruction of two groups of imaging planes including body and heart planes. Standard body planes include three orthogonal cuts in axial (transverse), coronal, and sagittal orientations. Heart planes also include three orthogonal planes in relation to the heart axes [1, 2]. Short-axis images, which correspond to the plane of the atrioventricular (AV) groove, are oblique and are oriented closer to the vertical than to the horizontal plane. Horizontal long-axis (four-chamber) views are double oblique planes perpendicular to both the interventricular septum and the AV plane of the heart. Vertical long-axis (two-chamber) views of the heart are parallel to the interventricular septum (Figure 1.1).
Everyone must be familiar with radiographic borders of the heart in different projections (Figure 1.2). On anterior projection, the right cardiac border is formed by the right atrium (RA), while the left cardiac border is formed by the left ventricle (LV). The right ventricle (RV) and the left atrium (LA) are superimposed structures and are not border-forming, and additional projections are required to review them. Diaphragmatic surface is formed by the RV. On the lateral projection, the anterior cardiac border is the RV, while the posterior cardiac border is composed of both the LV and the LA.
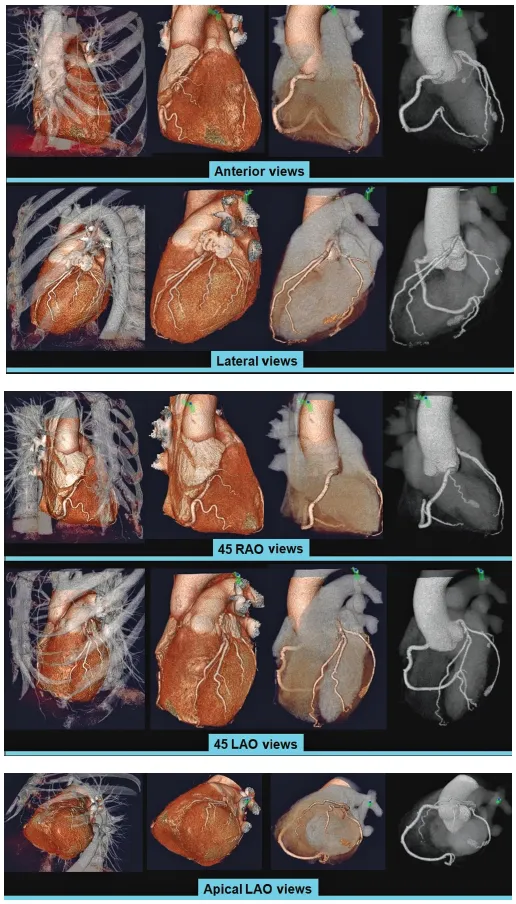
Anteriorly, the heart is covered by the sternum and the costal cartilages. The heart has an extensive diaphragmatic surface inferiorly (Figure 1.3). Posteriorly, the heart lies on the esophagus and the tracheal bifurcation, and bronchi that extend into the lung. The sternum lies anteriorly and provides rigid protection to the heart during blunt trauma.
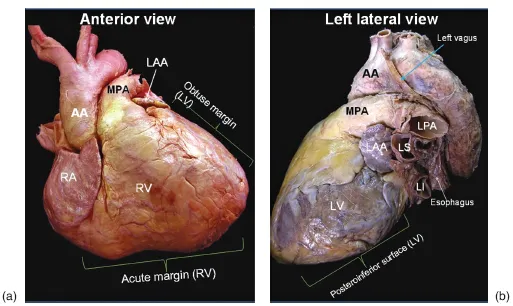
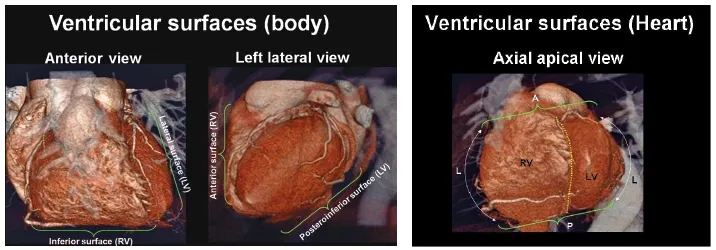
The true posterior surface of the heart is commonly termed the base of the heart, which is formed largely by the LA. The term “base of the heart” is not frequently used and is restricted to the “origin of the great vessels.” The inferior surface of the heart is also closely related to the diaphragm and should not be entirely called posterior. In supine position, along with elevation of the diaphragm, the lower surface of the heart largely faces inferiorly; however, in upright position, with full inspiration, the heart stands vertically and these walls face posteroinferiorly [1]. Because of the obliquity of the surfaces of the ventricles, the diaphragmatic surface of the RV is truly inferior and the diaphragmatic wall of the LV faces posteroinferiorly (Figures 1.3–1.5).
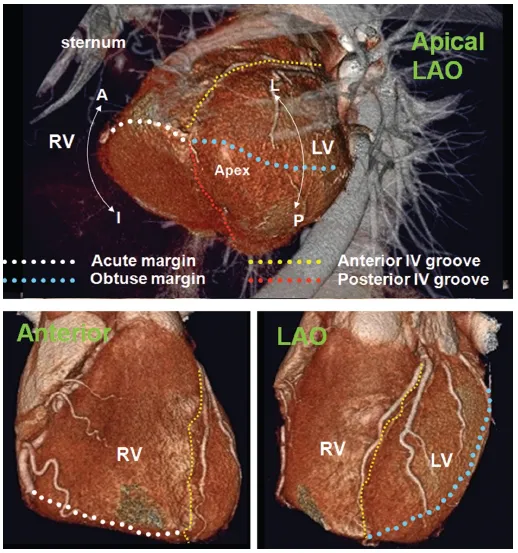
The heart is a three-sided pyramid located in the middle mediastinum. When viewed from its apex, the three sides of the ventricular mass are readily seen (Figure 1.5). Two of the edges are named. The acute margin lies inferiorly and describes a sharp angle between the sternocostal and diaphragmatic surfaces. The obtuse margin lies superiorly and is much more diffuse. The posterior margin is unnamed but is also diffuse in its transition.
The Right Atrium
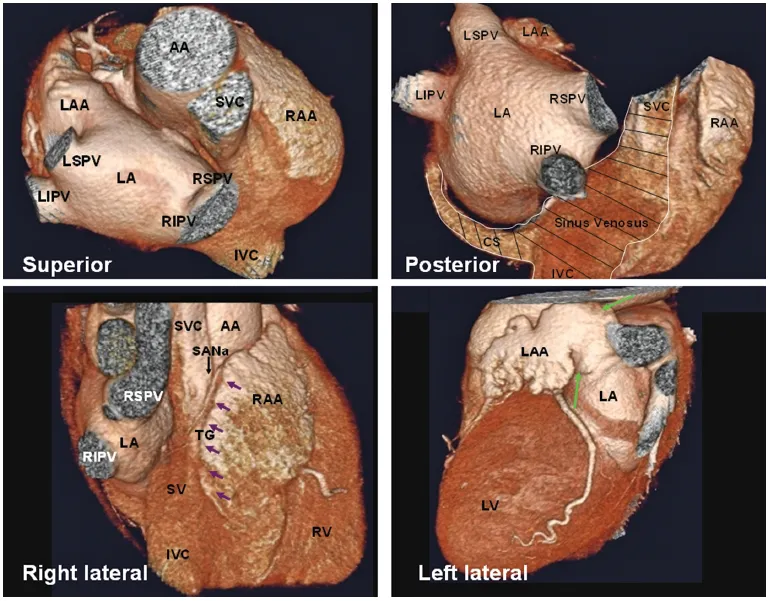
The RA is the chamber of the heart that receives systemic venous blood return from the superior vena cava (SVC) and inferior vena cava (IVC) and coronary venous return from the coronary sinus. Looking at three-dimensional images of the heart from the top, RA is positioned to the right and anteriorly, while the LA is situated to the left and mainly posteriorly [3] (Figure 1.6)
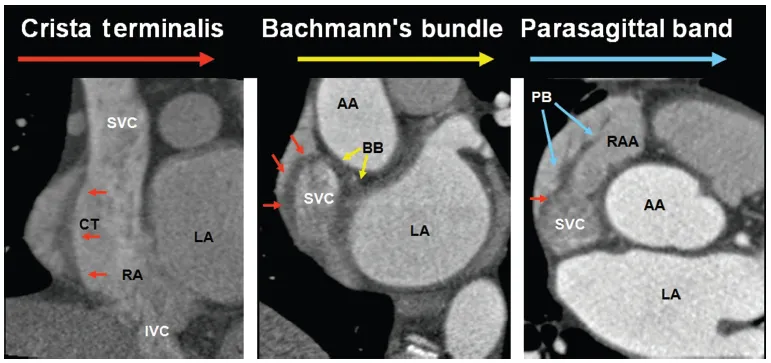
From a spatial point of view, the RA may be divided into lateral, medial, inferior, and posterior walls. The RA comprises three components: the appendage, the venous part (sinus venarum), and the vestibule [4, 5]. One of morphologic characteristics of the RA is the presence of the crista terminalis. This C-shaped muscular ridge separates the smooth-walled sinus venarum from the trabeculated appendage (the right half of the primitive atrium) [6]. The crista terminalis varies in size and extent in different individuals (Figure 1.7; see also Chapter 9, cardiac anatomy for electrophysiologic interventions). Another indicator of the right atrial morphology is a large, wide-based appendage (Figure 1.6). Some anatomists define the appendage as the anterosuperior protrusion of the body of the RA, an anatomic feature rather than an anatomic subdivision. The vestibule, also known as supravalvular lamina, is a smooth muscular rim surrounding the tricuspid orifice [1] (Figure 1.8). The pectinate muscles do not reach this area (Figure 1.5; see also Chapter 9). The right coronary artery (RCA) runs in the epicardial fat next to the vestibule.
Terminal groove is a fat-filled sulcus on epicardial side, which corresponds internally to crista terminalis (Figure 1.6, the right lateral view). The sinus node and terminal segment of sinoatrial (SA) node artery are located in this groove, close to the superior cavoatrial junction.
The sinus venarum is mainly located in the posterolateral wall of the RA between the SVC and IVC orifices [7] (Figure 1.6). From the third week after the development of the primitive heart tube, the primitive atria are separated from the sinus venosus by a segmentation termed the SA ring. The sinus venosus has two horns. The right horn gives rise to all the intercaval regions of the RA including the crista terminalis, the Eustachian ridge, and the Thebesian valve (Figure 1.6). The left horn gives rise to the coronary sinus [8]. The interatrial septum is located posteromedially.
The RA is home to important parts of the cardiac conduction system including the SA and the AV nodes (AVNs) [9–11]. The SA node (SAN) is a banana-shaped structure in the subepicardial side of superior cavoatrial junction, composed of cells slightly smaller than normal working cells (Figure 1.11; see also Chapters 9). It is the source of the cardiac impulse. Because of the vicinity of the sinus node to the epicardial surface, it may be damaged in selected cardiac surgeries or extensive pericardial diseases [9]. The SAN is supplied by the SAN artery. The SAN artery is usually, a single branch, arising from the proximal RCA (60%) or the left circumflex (LCx) artery (40%) (see Chapter 4 and 9 for details). In the majority of hearts, the SAN artery passes through the center of SAN [11] (Figure 1.9).
The AVN is located within the boundaries of Koch’s triangle near its apex. The triangle of Koch is an important anatomic landmark of the RA, which is commonly used for electrophysiologic studies (Figure 1.17; see also Chapter 9). This triangle is bordered posteriorly by the tendon of Todaro (fibrous extension from the Eustachian valve), anteriorly by the septal leaflet of the tricuspid valve, and inferiorly by the ostium of the coronary sinus (Figure 1.10). The size of Koch’s triangle is variable in different individuals. The apex of this triangle corresponds to the central fibrous body of the heart [12].
The AVN consists of a compact portion and an area of transitional cells. The compact portion lies over the central fibrous body [13] (Figure 1.19; see also Chapter 9). The AVN continues distally with the penetrating bundle of His. The AVN artery originates from the distal RCA (80–90%) and penetrates into the base of the posterior interatrial septum (inferior pyramidal space) at the level of crux of the heart in 80–87% of patients (Figure 1.11). In the remaining, it originates from the distal LCx artery [14–16].
The inferior wall of the RA is a complex area with several important anatomic landmarks [7,17]. The IVC and the coronary sinus connect to this portion of the RA. The Eustachian valve guards the anterior margin of the IVC. It is usually membranous and variably developed (Figure 1.26; see also Chapter 9). It may look fenestrated or contain muscles. Usually it inserts medially to the Eustachian ridge or sinus septum, which is the border between the oval fossa and the coronary sinus. The medial border of the Eustachian valve continues as a tendon of Todaro that runs in the musculature of the Eustachian ridge. Mistakenly, the valve may be sutured to the anterior rim of an atrial septal defect at the time of shunt repair. Laterally, the Eustachian valve merges into the crista terminalis. In some cases, it is large, posing an obstacle to pass a catheter.