![]()
Chapter 1
Introduction
Penny Simkin, BA, PT, CCE, CD(DONA), and Ruth Ancheta, BA, ICCE, CD(DONA)
Some important differences in maternity care between the United States, the United Kingdom, and Canada
Notes on this book
Changes in this third edition
Material on epidurals
Conclusion
References
Labor dystocia, dysfunctional labor, failure to progress, arrest of labor, arrested descent—all these terms refer to slow or no progress in labor, which is one of the most vexing, complex, and unpredictable complications of labor. Labor dystocia is the most common medical indication for primary cesarean sections. Dystocia also contributes indirectly to the number of repeat cesareans, especially in countries where rates of vaginal births after previous cesareans (VBAC) are low. In fact, The American College of Obstetricians and Gynecologists (ACOG) estimates that 60% of all cesareans (primary and repeat) in the United States are attributable to the diagnosis of dystocia.1 Thus, reducing the need for cesareans for dystocia is a strategic way to reduce the overall cesarean rate. Prevention of dystocia also reduces the need for many other costly and risky corrective obstetric measures and spares numerous women from the discouragement and disappointment that often accompany a prolonged or complicated birth.
The possible causes of labor dystocia are numerous. Some are intrinsic:
- The powers (the uterine contractions)
- The passage (size, shape, and joint mobility of the pelvis and the stretch and resilience of the vaginal canal)
- The passenger (size and shape of fetal head, fetal presentation and position)
- The pain (and the woman’s ability to cope with it)
- The psyche (anxiety, emotional state of the woman).
Others are extrinsic:
- Environment (the feelings of physical and emotional safety generated by the setting and the people surrounding the woman)
- Ethnocultural factors (the degree of sensitivity and respect for the woman’s culture-based needs and preferences)
- Hospital or caregiver policies (how flexible, family- or woman-centered, how evidence based)
- Psychoemotional care (the priority given to nonmedical aspects of the childbirth experience)
Please see Michael Klein’s Foreword to the second edition (page xviii) for his discussion of factors influencing labor progress.
The Labor Progress Handbook focuses on prevention, differential diagnosis, and early interventions to use with dysfunctional labor (dystocia). The emphasis is on relatively simple and sensible care measures or interventions designed to help maintain normal labor progress and to manage and correct minor complications before they become serious enough to require major interventions. We believe this approach is consistent with worldwide efforts, including those of the World Health Organization, to reserve the use of medical interventions for situations in which they are needed: “The aim of the care [in normal birth] is to achieve a healthy mother and baby with the least possible level of intervention that is compatible with safety.”
2
The suggestions in this book are based on the following premises:
- Progress may slow or stop for any of a number of reasons at any time in labor—prelabor, early labor, active labor, or during the second or third stage.
- The timing of the delay is an important consideration when establishing cause and selecting interventions.
- Sometimes several causal factors occur at one time.
- Caregivers and others are often able to enhance or maintain labor progress with simple nonsurgical, nonpharmacologic physical and psychological interventions. Such interventions have the following advantages:
- compared to most obstetric interventions for dystocia, they carry less risk of harm or undesirable side effects to mother or baby.
- they treat the woman as the key to the solution, not the key to the problem.
- they build or strengthen the cooperation between the woman, her support people (loved ones, doula [trained labor support provider]), and her caregivers.
- they reduce the need for riskier, costlier, more complex interventions.
- they may increase the woman’s emotional satisfaction with her experience of birth.
- The choice of solutions depends on the causal factors, if known, but trial and error is sometimes necessary when the cause is unclear. The greatest drawbacks are that the woman may not want to try these interventions; they sometimes take time; or they may not correct the problem.
- Time is usually an ally, not an enemy. With time, many problems in labor progress are resolved. In the absence of clear medical or psychological contraindications, patience, reassurance, and low or no risk interventions may constitute the most appropriate course of management.
- The caregiver may use the following to determine the cause of the problem(s):
- objective observations: woman’s vital signs; fetal heart rate patterns; fetal presentation, position, and size; cervical assessments; assessments of contraction strength, frequency, and duration; membrane status; and time
- subjective observations: woman’s affect, description of pain, level of fatigue, ability to cope with self-calming techniques.
- direct questions of the woman and collaboration with her in decisions regarding treatment:
“What was going through your mind during that contraction?”
“Please rate your pain during your previous contraction.”
“Why do you think labor has slowed down?”
“Which options for treatment do you prefer?”
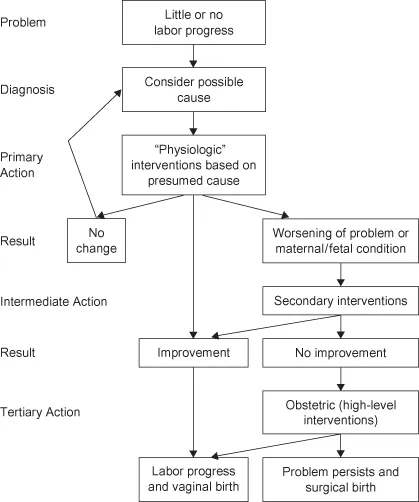
- Once the probable cause and the woman’s perceptions and views are determined, appropriate primary interventions are instituted and labor progress is further observed. The problem may be solved with no further interventions.
- If the primary interventions are medically contraindicated or if they are unsuccessful, then secondary, relatively low-technology interventions are used, and only if those are not successful are the tertiary, high-technology obstetric interventions instituted under the guidance of the doctor or midwife.
Chart 1.1 illustrates the approach described in this book. Other, similar flow charts appear throughout this book to illustrate the application of this approach to a variety of specific causes of dysfunctional labor.
Many of the interventions described here are derived from the medical, midwifery, nursing, and childbirth education literature. Others come from the psychology, sociology, and anthropology literature. We have provided references for these, when available. Some suggestions have come from the extensive experience of nurses, midwives, doctors, and doulas. Many are applications of physical therapy principles and practices. Some items fall into the category of “shared wisdom,” where the original sources are unknown. We apologize if we neglect to mention the originator of an idea that has become sufficiently widespread to fall into this category. Finally, some ideas originated with one, some, or all of the authors who have used them successfully in their work with laboring women.
With today’s emphasis on evidence-based practice, many rather entrenched maternity care customs are falling out of favor because they have been proven ineffective or harmful. Routine practices, such as enemas, pubic shaving, continuous electronic fetal monitoring, maternal supine and lithotomy positions in the second stage of labor, episiotomy, immediate clamping of the umbilical cord, and routine suctioning of the baby’s airway after birth are examples of forms of care that became widespread before they were scientifically evaluated. Then, once well-controlled trials of safety and effectiveness had been performed and the results combined in meta-analyses, these common practices were found to be ineffective and to increase risks.3
Where possible, we will base our suggestions on scientific evidence and will cite appropriate references. However, numerous simple and apparently risk-free practices have never been scientifically studied. Some of these are based on an understanding of the emotional and physiologic processes taking place during childbirth. Others are applications of anatomy, kinesiology, and body mechanics to enhance the relationships between such separate but interdependent forces as pelvic shape, maternal posture, fetal position and station, uterine activity, and the force of gravity. Still others are based on a recognition of the importance of each laboring woman’s personal and cultural values.
Some of the strategies suggested in this book will lend themselves to randomized controlled trials, while others may not. Perhaps readers will gather ideas for scientific study as they read this book and apply its suggestions.
SOME IMPORTANT DIFFERENCES IN MATERNITY CARE BETWEEN THE UNITED STATES, THE UNITED KINGDOM, AND CANADA
This book is being published simultaneously in North America and the United Kingdom, where the approaches to maternity care are quite different from one another. It may surprise the reader to learn about some of those differences, and it may also be interesting to learn that practices that are considered essential for safety in one country are considered ineffective or archaic in another. We hope that one indirect effect of our book will be to encourage a willingness to reconsider practices that are either entrenched or avoided in one’s own workplace.
Table 1.1 compares some basic features of maternity care between the United States, Canada, and the United Kingdom. Because of such differences in maternity care as those listed in Table 1.1, the willingness to introduce new practices and the power to do so will vary among caregivers in different countries. We hope our readers will begin to use the simplest, most innocuous measures immediately and to educate themselves and change policies where necessary.
Table 1.1. Comparison of maternity care in the United States, Canada, and the United Kingdom
NOTES ON THIS BOOK
This book is directed toward midwives, nurses, and doctors who want to support and enhance the physiologic process of labor with the objective of avoiding complex, costly, more risky interventions. It will also be helpful for students in obstetrics, midwifery, and maternity nursing; for childbirth educators who can teach many of these techniques to expectant parents; and for doulas, who are qualified and skilled in the use of many of the techniques. The chapters are arranged chronologically according to the phases and stages of labor.
Because a particular maternal position or movement is useful for the same problem during more than one phase of labor, we have included illustrations of these positions in more than one chapter. This will allow the reader to find position ideas at a glance when working with a laboring woman. Complete descriptions o...