Nowadays, single-retainer metal-ceramic and all-ceramic resin-bonded fixed dental prostheses (RBFDPs) often present a truly minimally invasive alternative to singletooth implants or other conventional prosthetic methods. Their excellent clinical outcome has been proven by several recently published long-term studies.With the growing body of evidence showing that implants placed in the esthetic zone of younger patients present a high risk of esthetic problems in later years, RBFDPs made from zirconia ceramics are experiencing a great renaissance.This book presents, concisely and precisely, what has to be considered and what must be avoided in order to be successful with single-retainer RBFDPs replacing incisors. Although the method is technically sensitive, it is simple and extremely reliable when adequate procedures are employed. In the meantime, even the replacement of canines and premolars appears to be promising if the principles outlined in this book are applied. Numerous highquality figures detail the procedures for metal-ceramic and all-ceramic RBFDPs. Many illustrated cases, some with 20 and more years of follow-up, document the development of the success story of RBFDPs.
eBook - ePub
Resin-Bonded Fixed Dental Prostheses
Minimally invasive – esthetic – reliable
- 264 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
About this book
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
Chapter 1
Why RBFDPs evolved to a single-retainer design
Buonocuore’s20 development of the acid-etch technique for enamel 60 years ago provided the basis to achieve high and durable enamel bonding using dental resins (Fig 1-1). In the 1970s, artificial teeth were initially bonded with composite resin to adjacent abutment teeth for anterior tooth replacement37 using the acid-etch technique. However, the longevity of these purely resin-based restorations was rather limited.
Today, extracted natural or artificial teeth can still be adhesively bonded in the same way to serve as long-term provisional restorations, e.g. when inflamed tissues in the alveolar ridge need time to heal prior to the fabrication of the final prostheses. It requires no great effort to shorten an extracted tooth by cutting off its root and to bond it back adhesively. However, after removing the root the remaining crown should be sealed on its cervical end using a dentin adhesive, and by using a tooth-colored composite resin, an ovate pontic basis is formed. The ovate pontic should reach 2 to 3 mm into the extraction socket and support the marginal gingiva circumferentially (immediate pontic technique, compare with Fig 5-11). In this way, the blood coagulum in the extraction socket is also protected. In the presented case (Figs 1-2 to 1-9), the resin bonding of the extracted and shortened tooth was reinforced using a polyethylene fiber net (Ribbond). Figure 1-9 presents the restoration after 14 years of clinical service. This case is an example of the excellent durability of bonding to enamel. Mostly, such long-term provisional restorations will fail after several years of clinical service due to a fracture of the elastic fiber-reinforced resin bonding. However, at this stage the hard and soft tissues have healed, so that either a final resin-bonded fixed dental prosthesis or a single tooth implant can be used for the final prosthetic restoration.
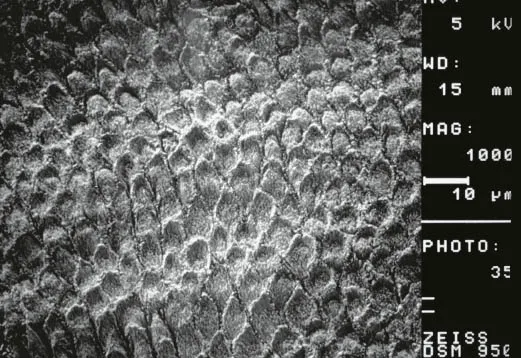
Fig 1-1Enamel etching pattern after etching with phosphoric acid (scanning electron microscopic photo at 1000× original magnification).

Fig 1-2Labial view of the hopeless tooth 32 (situation after repeated unsuccessful apicoectomies done elsewhere).

Fig 1-3Fabrication of an incisal-positioning splint prior to extraction of tooth 32.

Fig 1-4Situation after extraction of tooth 32. Care was taken to ensure complete filling of the extraction socket with blood.

Fig 1-5Basal view of the removed tooth revealing an untreated lingual root canal, and a crack in the labial canal wall.

Fig 1-6Reshaping the root portion with adhesive techniques and composite resin into an ovate pontic shape.
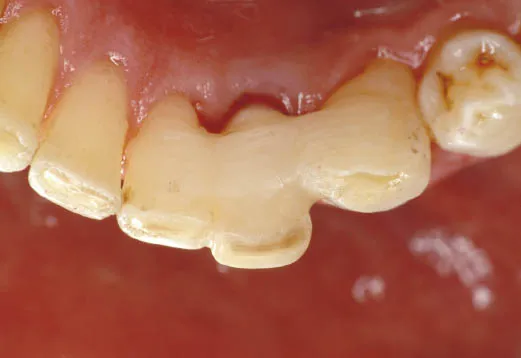
Fig 1-7Occlusal view of tooth 32 that was adhesively fixed with composite resin reinforced with a lingual fiber net under rubber dam isolation.

Fig 1-8Labial view of tooth 32 after complete healing.

Fig 1-9Status 14 years after reinsertion of the extracted reshaped tooth [Source: CDT Matthias Hasselberg, Eckernförde, Germany].
These composite resin fixed teeth did not provide good long-term results on a regular basis. To improve longevity, Rochette80 suggested using metal-based resin-bonded fixed dental prostheses (RBFDPs) with two retainer wings for anterior tooth replacement. Macromechanical retention for the metal retainer wi...
Table of contents
- Cover
- Title
- Copyright
- Dedication
- Preface
- Acknowledgment for the English edition
- Acknowledgment for the German edition
- Author
- Contents
- Chapter 1 Why RBFDPs evolved to a single-retainer design
- Chapter 2 When single-retainer RBFDPs are useful
- Chapter 3 When single-retainer RBFDPs (alone) are not useful
- Chapter 4 Excellent longevity of single-retainer RBFDPs
- Chapter 5 Advantages and disadvantages of single-retainer RBFDPs
- Chapter 6 When RBFDPs should bond long term
- Chapter 7 Adequate diagnosis and treatment planning are essential
- Chapter 8 Pretreatment is of utmost importance
- Chapter 9 Metal-ceramic RBFDPs – concise
- Chapter 10 All-ceramic RBFDPs – detailed
- Chapter 11 To splint or not to splint – that is the question
- Chapter 12 Replacement of canines and premolars
- Chapter 13 Aftercare: prevent problems – solve problems
- Chapter 14 What you have to do to make it go wrong – the 10 most common mistakes in the application of RBFDPs
- Chapter 15 Appendix
- Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Resin-Bonded Fixed Dental Prostheses by Matthias Kern in PDF and/or ePUB format, as well as other popular books in Medicine & Dentistry. We have over 1.5 million books available in our catalogue for you to explore.