![]()
Chapter 1
An introduction to the professions
Learning outcomes
By the end of Chapter 1, you should be able to:
- understand the key differences between nursing and midwifery
- recognise the essential skills and attributes required of a nurse or midwife and why they are important
- begin to relate those skills and attributes to your own
- appreciate the impact a nurse or midwife has on the well-being and experiences of healthcare consumers
- confidently identify your chosen professional route and continue relevant research using the resources provided
Introduction
This opening chapter explores the nature of the nursing and midwifery professions, what it means to be a nurse or midwife, and what sort of essential skills and attributes are required. Rather than do this as a lengthy, descriptive account that can tend to be rather dry, I have instead enlisted the help of colleagues who between them have created rich and varied accounts of their professional lives and the nature of the patients/clients they serve. These should serve to illuminate the professions and can be placed in further context later on in the chapter by reading the perspectives of students themselves.
Why be a nurse or midwife?
Chapter 1 is important in helping towards the development of knowledge and understanding of your chosen profession. As you will discover in Chapter 3, being able to articulate a clear and objective motivation for application to a nursing or midwifery degree programme is key to being successful at the shortlisting stage. This section will therefore focus on the essential characteristics of nurses and midwives, illuminated by reflections on practice from clinicians, their typical ‘life in a day’ diaries, and by the perspectives of nursing students. Firstly, it is important to place this within a broad historical context as both people and policies continue to have a significant influence on healthcare, and therefore practitioners, in contemporary Britain.
There are a number of excellent texts available that outline the historical development of the professions – details of these are provided in the next section. As part of the research into your chosen profession and certainly before you apply for a place on a highly competitive course, you would be wise to look at some of these first. Not only will this background reading be interesting and relevant to your application, it is an important step in the decision-making process. Although a detailed history of the professions is outside the remit of this book (and has been done very well by many others), it may be of use to you to complete a historical timeline of important events. Your background reading, guided by the references provided, will help illuminate these events and enrich your understanding of the profession you have chosen to apply for.
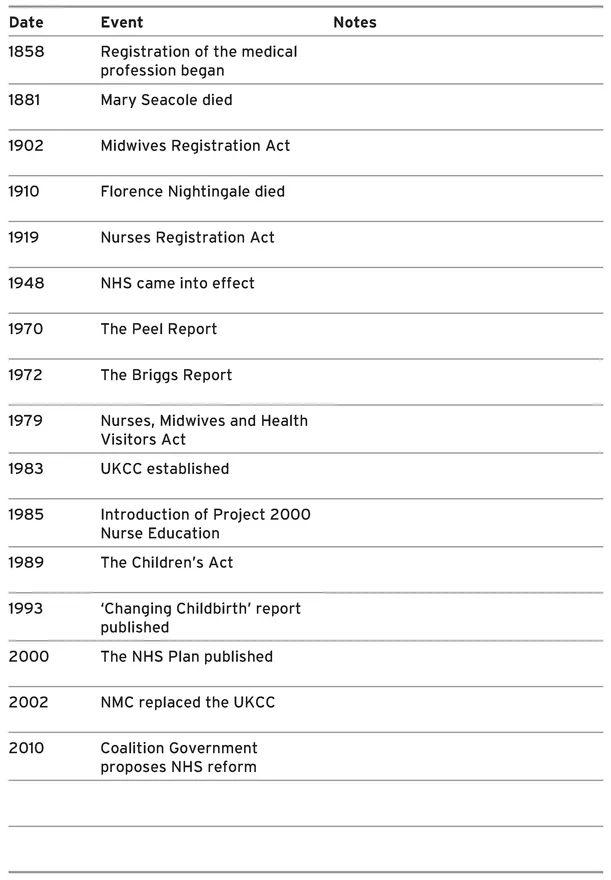
Historical timeline
The key resources provided in Box 1.1 will help you understand the events on the timeline and to complete the blank sections in Activity 1.1. Completing this activity will provide valuable information for future reference, as well as being a way of developing your information searching skills. Spaces have been left at the end of the table for you to add anything else that you consider relevant during completion of the timeline. As a midwife teacher, I know that information gathering is an essential skill for undergraduate midwifery and nursing students to acquire early on in their studies – so why not start now.
Box 1.1 Timeline resources
Lowis G, van Tejilingen E, McCaffery P, Porter M (eds) (2004) Midwifery and the Medicalisation of Childbirth: Comparative Perspectives. Nova Science Publishers Inc.
http://www.bbc.co.uk/radio4/womanshour/02/2009_24_tue.shtml
BBC Radio Woman’s Hour broadcast about the history of district nursing.
http://www.nmc-uk.org/About-us/The-history-of-nursing-and-midwifery-regulation/
NMC page looking at the history of nursing and midwifery regulation.
http://www.nursing.manchester.ac.uk/ukchnm/
UK Centre for the History of Nursing and Midwifery.
Activity 1.1
Historical timeline
Research the events listed and then make notes in the spaces available.
What is it like being a nurse or midwife?
In order to answer this question, I have drawn together a number of personal reflections and diary extracts from colleagues who have amassed a vast number of years’ experience between them as healthcare practitioners. These will offer the reader a ‘bird’s-eye’ view of what makes a nurse or midwife tick.
Names of clients/patients are pseudonyms in order to protect confidentiality.
Reflection 1.1
Sarah Snow, Midwife
My career in healthcare began by accident in 1984. As a naïve 18-year-old, I had no real idea of what I wished to do with my life – nursing seemed as good a job as any, although I remember that my Dad really wanted me to work in a bank. In those days, dual registration was considered to be an excellent career move and I therefore embarked on a midwifery pathway after some experience as a Staff nurse. I have little memory of my training, other than being told off on a regular basis – in those days, nursing and midwifery was strictly hierarchical and regimental. I frequently breached the ‘rules’ by making friends with the night sisters, or having my hair longer than the top of my uniform collar. It’s really only the experiences I subsequently enjoyed as a qualified midwife that began to shape my philosophy about the care of women during childbirth and the importance of looking after student midwives.
In 1994, I was working on the delivery suite of a maternity unit that handled around 1,500 births per year. I had been qualified as a midwife for four years and was just starting to have the confidence to assert myself more as the midwife I wanted to be. I believed, and still do, that women should do what feels right for them during the births of their babies, but was also acutely aware that women’s wishes were frequently ignored or sidetracked within the maternity services. I was happy working within this maternity unit and felt supported and valued in my practice most of the time. It was also a significant time in my personal life – I got married and met my closest friend through working at this unit. In addition, two of my current teaching colleagues who I respect greatly were also midwives within the unit at this time.
During one particular shift, I looked after Jill, who was in labour having her second baby. I hadn’t met Jill before – this was usual – and therefore had limited time to foster an effective relationship with her. As we got to know each other a little, Jill told me that her first experience had been mostly negative – she felt little choice had been offered, and her birth plan not respected. We talked about Jill’s wishes for the delivery of this baby and she asked me, very tentatively, if she could give birth standing up. I had not helped women in this position before, and knew that many of my colleagues were sceptical about any position other than being on a delivery bed, but I was very happy to support Jill in her wish – it really didn’t seem to be a big deal for me.
A few hours later, Jill delivered her baby girl standing up with me crouching at her feet ready to catch the baby. The baby was born very quickly and easily because of the upright position – I learnt for the next time to encourage women to lean forwards slightly to slow down the birth a little – and Jill was absolutely delighted and full of praise for me. I remember thinking ‘why is she so grateful?’ because all I had done was support Jill in her decision-making. Of course, as I got older and somewhat wiser, I realised that my small contribution to this woman’s birth was hugely significant in terms of her choice and control. This significance was reinforced during the births of my own children, where the need to emerge emotionally intact from the experience was hugely important to me.
Later, I received a card from Jill that thanked me for making her birth ‘so unfrightening’. There was also a gift – a beautiful Art Deco mug that sits on my shelves still, 16 years later. Seeing it there serves as a beacon of light in my ongoing practice as a midwifery educator. It takes courage to support women’s choices within hostile birth environments, especially with the knowledge that the application of that courage can have life-long consequences.
Reflection 1.2
Pete Stenson, Nurse Specialist, Sexual Health
It is not uncommon for patients to ask ‘what made you choose this job?’ Perhaps the patient would like to hear that it was a calling and that the nurse ‘just wanted to help sick people’ when in fact the reason may be geographical: ‘I only live around the corner’; financial: ‘this job pays more’; or social: ‘the hours fit in with childcare’. Sometimes, patients state ‘Oh I couldn’t do your job’. I’ve never been quite sure if this is supposed to make nurses feel better about their career choice.
Like many nurses, I was directly influenced in my choice by my experience as a student nurse. In the late 1960s, it was felt by nurse tutors that it was inappropriate for male students to have placements on the gynaecological wards, so I was sent along to what was then called the ‘VD Clinic’. The clinic was to be found in the basement next to the boiler house and the entrance was separate from the main outpatient entrance. The small door in the wall had a sign above it that proclaimed ‘Chest Clinic’. I thought the rather dingy setting did not bode well for a six-week placement. Nothing could have been further from the truth. The inside of the clinic was clean and bright and the staff happy and smiling. I reported to Mr Jack Edwards, the nurse/technician who was in charge of the clinic. Not only was he very welcoming, he immediately gave me a tour of the clinic and introduced me to the other staff, including the consultant who also welcomed me to the clinic. In my previous ward experience, I don’t think that a consultant had ever spoken directly to me, so this was a novel experience. The training programme was explained to me – it included some real hands-on stuff like microscopy, issuing medicines, requesting microbiology tests and taking blood; the latter were tasks at that time only undertaken by doctors. Being the only student, I was given individual tuition and I responded by even reading about sexually transmitted diseases in my own time!
I followed Jack Edwards around for the first few weeks and was amazed by his in-depth knowledge – on occasion, even the consultant sought his opinion. The range of duties he was able to carry out was extensive and he took decisions about the diagnosis and what treatment the patient was to receive. But above all I was struck by his kindness to the patients, many of whom were devastated when told that they had a sexually acquired infection. At that time, the stigma and risks surrounding these diseases were very real.
My six happy weeks in the clinic soon came to an end. Before I left, Jack took me to one side to explain all the benefits that working in the clinic would have once I had completed my training – his memorable comment was that ‘as long as people had sex I would always have a job’. He painted a rosy picture of life in what he called the ‘Cinderella service’. I took him at his word; I started work in sexual health in the early 1970s and have continued in the same job for 38 years. Everything Jack had predicted turned out to be true; sexual health nurses have a good deal of autonomy and nurse led services now make up the majority of clinic appointments.
It is quite trendy to work in sexual health now and I have enjoyed introducing numerous students to the delights of sexual health nursing. I had the honour of working with Jack for five years until he retired aged 81. Many years later, when we moved to new premises I had the pleasure of naming the new clinic after him.
Life-in-a-day 1.1
Ali Spencer, Critical Care Outreach Sister
I am part of a Critical Care Outreach Team in a District General Hospital. The team was set up 11 years ago as a government initiative to provide support and education to general ward nurses looking after deteriorating patients on general wards. It is made up of senior nurses who have all had several years of Critical Care experience and who are also experienced in teaching and supporting other nurses.
It is a fantastic job as it allows me to care for really sick patients and to teach other nurses, which are both passions of mine!
To give you some insight into my role I thought I would share a few hours of a typical day with you and hopefully you’ll agree that it is interesting and exciting.
It is Saturday morning and I arrive for work at 8.40 am to find my partner in crime for the day waiting for me in the office. He has already taken handover from the Night Nurse Practitioner who has asked him to see one patient that she had been called to overnight. He has also been to the Critical Care Unit to find that two patients were discharged to general wards overnight. Our hours of service are 8.00 am to 5.00 pm every day and we work closely with the Night Nurse Practitioners so that nurses can be supported caring for sick patients 24 hours a day. We see all patients who are discharged from the Critical Care Unit and also take referrals from ward nurses, specialist nurses and doctors. Once we have identified and allocated the patients to be seen, we set off to assess them. We carry one pager each that allows doctors and nurses to contact us to refer sick patients, and also the Medical Emergency pager as we form part of that team also.
My first patient is a gentleman who was discharged from the Critical Care Unit yesterday afternoon to a general surgical ward. He is 72 years old and had undergone bowel surgery for a tumour. He required critical care support because he had a history of cardiac disease and stroke but he had an uneventful recovery and now requires follow up from Outreach.
I arrived on the ward and introduced myself to him and to the nurse looking after him, before carrying out a comprehensive assessment including observations and test results. I found him to be recovering well and only needed to reduce his oxygen and advise on frequency of observations before reassuring him of his good progress. He was quite straightforward as he had only been a patient on the unit for 24 hours. I discharged him to the care of the ward staff but reassured them that they could contact me about him if they became concerned about his condition.
Some patients are on the Critical Care Unit fo...