- 264 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
Working with Dysphagia
About this book
This practical text is indispensable to all clinicians working with dysphagia and is suitable for those involved in a range of settings and with a diversity of client groups. With its perspective on everyday working practice, "Working with Dysphagia" fills a gap in an area where practical and workable material is much sought after. This book is a useful resource for all therapists, ranging from students to specialist, as the practical assessment approach and comprehensive management strategies are supported throughout with references of recent relevant research.
Tools to learn more effectively

Saving Books

Keyword Search

Annotating Text

Listen to it instead
Information
Chapter 1:
The Normal Swallow
◆ Neuroanatomy and Anatomy of the Normal Swallowing Process in Adults
◆ Physiology of the Normal Swallowing Process in Adults
◆ Factors Affecting the Normal Swallow
◆ Swallowing Reflexes
Neuroanatomy and Anatomy of the Normal Swallowing Process in Adults
This section describes the basic neuroanatomy and anatomy of swallowing. The content has been selected to ensure that the reader can fully comprehend the physiology, assessment and management of swallowing (and its disorders) which follow.
Neuroanatomy
The cranial nerves, seven of which are vital in controlling swallowing, provide both a motor function and sensory information. While they are crucial to the swallowing process, clinicians may experience difficulty in retaining details of their innervation and function. Functional assessments look at the whole swallowing process, rather than individual nerve responses.
In specific cases (such as those resulting from anoxia, or following head and neck surgery) it may be appropriate to look in detail at individual cranial nerves. Therefore, a basic summary of their sensory and motor functions is provided in Table 1.1. The neural control of swallowing is covered later in this chapter.
Anatomical structures
Details of the important anatomical structures are provided in this section. The specific muscles are not detailed, since they are of significance in a functional dysphagia assessment only if one is dealing with a client who has undergone head and neck surgery. This is not the remit of this book. The important anatomical structures are shown in Figure 1.1.
The oral cavity
The oral cavity is separated from the nasal cavity above by an anterior bony hard palate, and a soft (muscular) palate posteriorally. The soft palate is relaxed, allowing an exchange between the two cavities during respiration, but closes during swallowing to prevent nasal regurgitation. The anterior section of the hard palate, directly behind the upper teeth, is known as the alveolar ridge.
Table 1.1 Cranial Nerves and their Function
| Cranial Nerve | Sensation | Motor Function |
| CN I, olfactory | Smell | |
| CN V, trigeminal | General sensation from the face and muscles of mastication, anterior ⅔ of tongue | Mandibular movement, elevates soft palate, elevation and anterior movement of larynx |
| CN VII, facial | Salivation and taste (anterior ⅔ tongue), soft palate | Muscles of facial expression, elevation of hyoid and tongue base |
| CN IX, glossopharyngeal | Posterior ⅓ of tongue, soft palate, faucal arches, mucous membrane of pharynx | Stylopharyngeous muscle |
| CN X, vagus | Larynx, base of tongue, softStylopharyngeousmuscle and epiglottis, trachea, regulation of depth of respiration and control of blood pressure, nausea | Pharyngeal constrictors, cricopharyngeus, vocal folds |
| CN XI, accessory | From X via XI: soft palate, pharynx, tionand | |
| CN XII, hypoglossal | Intrinsic and extrinsic tongue muscles, mandible, hyoid and larynx |

Figure 1.1 Lateral view of the head and neck
The teeth arise from (or dentures attach to) an upper and lower jaw, the maxilla and mandible. The latter is mobile. Externally the jaws are bounded by the cheeks and lips, with the areas between these structures termed the sulci (lateral and anterior).
Within the oral cavity the muscular tongue is the most important structure. The oral section of the tongue includes the tip, blade and back. The body of the tongue sits on the hyoid bone, which is suspended from the oral cavity by the muscles of the floor of the mouth.
There are three pairs of major salivary glands within the oral cavity – the parotids, sublinguals and submandibulars. Further details of saliva production and function are provided in Chapter 6 ‘Oral Stage Management’. Final important markers in the oral cavity are the anterior faucal arches situated in front of the palatine tonsils (see Figure 1.2). These small areas are considered important in triggering the pharyngeal stage of the swallow.
The larynx
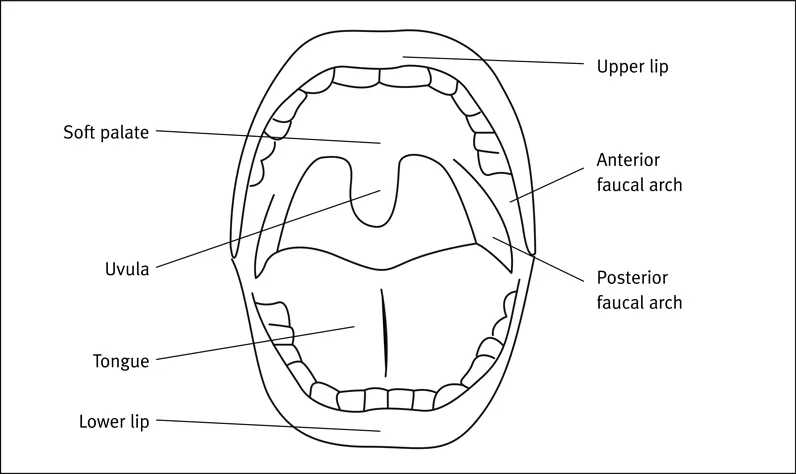
Figure 1.2 Anterior and posterior faucal arches
The cartilaginous larynx is suspended from the hyoid bone by the extrinsic laryngeal muscles. Therefore, if the hyoid elevates, the larynx must also rise, unless it is stabilised by musculature within the neck or shoulders. Situated in front of the hypopharynx, the larynx consists of the epiglottis, the thyroid cartilage, the cricoid cartilage and a number of intrinsic and extrinsic muscles (see Figure 1.3). The trachea is below the larynx.
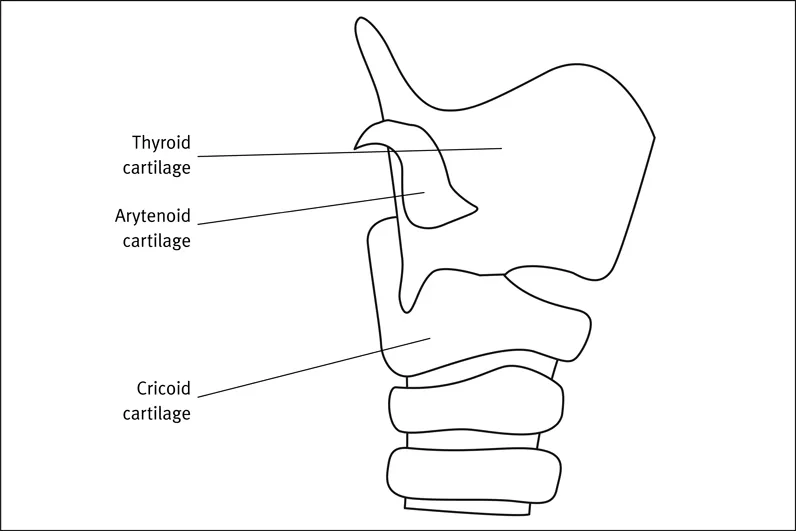
Figure 1.3 The laryngeal cartilages
Of greatest significance in the evaluation of swallowing disorders are (a) the valleculae, the wedge-shaped spaces at the base of the tongue on each side of the epiglottis, and (b) the false vocal folds and the true vocal folds (cords), lying within the thyroid cartilage (see Figure 1.4).
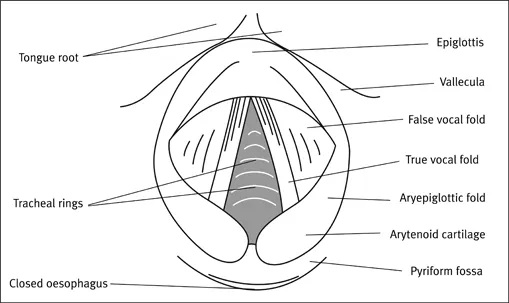
Figure 1.4 Interior of larynx
The pharynx
The pharynx can be divided into three areas: (a) the nasopharynx, which lies above the soft palate, (b) the oropharynx, lying posterior to the oral cavity, and (c) the hypopharynx, or lower portion of the pharynx.
Three muscular constrictors (superior, medial and inferior) form the posterior and lateral walls of the pharynx, attaching to structures situated anteriorly. These anterior bony and soft tissues are the soft palate, the tongue base, the mandible, the hyoid bone, and the thyroid and cricoid cartilages. At the point where the inferior constrictor attaches to the sides of the thyroid cartilage, bilateral spaces known as the pyriform fossae or pyriform sinuses are formed.
Directly below the pyriforms, the pharynx is closed from the oesophagus by the cricopharyngeus muscle (also known as the cricopharyngeus, the upper oesophageal sphincter, the UES, the pharyngo-oesophageal sphincter, cricopharyngeal sphincter or the PE segment).
The oesophagous
Situated behind the trachea, the oesophagus is a collapsed muscular tube, averaging 24cm in length. Closure is maintained by the cricopharyngeal muscle at the top and the lower oesophageal sphincter (or LES) at the bottom.
Physiology of the Normal Swallowing Process in Adults
Speech and swallowing – what is the relationship?
The premise of this book is that there is no relationship between the processes of speech and swallowing, other than shared anatomical structures. Kennedy et al (1993) reported, ‘In patients with cerebrovascular accidents, swallowing or speech may improve independently of each other (Netsell, 1986). In Parkinson’s disease severe dysarthria may exist with minimal or no dysphagia and the reverse (Sarno, 1968; Duvoisin, 1982). These observations are consistent with Netsell’s (1986) suggestion that there are specialised and differentiated neurones for speech and swallowing acts…. Thus, though both behaviours share the same anatomical structures, the actions of each are controlled by different command centres. At a clinical level this suggests that assessing one dysfunction in patients with neurological swallowing and communication difficulties may tell us little of the other.’
The stages of swallowing
The swallowing process consists of four stages: the oral preparatory, oral, pharyngeal and oesophageal. In reality, these stages do not occur in as discrete a way as detailed below; instead, the process is very rapid, with some overlap.
Oral preparatory stage
The level of preparation is dependent on the consistency of the material (known as the bolus) to be swallowed – solid, semi-solid or fluid. Fluid includes saliva. This is a fully voluntary stage, but where does it begin? When one picks up food or a drink, or when the bolus passes the lips? An increasing number of authors (including Leopold & Kagel, 1997) are proposing five stages, including an earlier, pre-oral ingestion stage. Clinical experience indicates that the more one can do to ensure that a person is ready to eat or drink and can participate in the self-feeding process, the more normal the oral preparatory and subsequent stages of swallowing. This point will be discussed further below. Influences on the pre-oral stage include state of hunger and thirst; visual and olfactory information; emotional state; milieu of the meal; societal influences; taste (see Figure 1.5); texture; motor skills, including utensil use; hand-mouth coordination; posture; eating rate. Thus the oral preparatory stage takes a variable amount of time.
Saliva is an essential component of this stage. It performs a number of functions – dental and mucosal protection, maintenance of oral pH, antimicrobial action – but most relevant to preparing the bolus for swallowing is its ability to lubricate and assist wi...
Table of contents
- Cover
- Half Title
- Title
- DEDICATION
- Contents
- List of Figures and Tables
- Acknowledgements
- Foreword
- Introduction
- Chapter 1 The Normal Swallow
- Chapter 2 Respiration and Aspiration
- Chapter 3 Subjective Assessment
- Chapter 4 Objective Assessment
- Chapter 5 General Issues in Management
- Chapter 6 Oral Stage Management
- Chapter 7 Pharyngeal Stage Management
- Chapter 8 Tracheostomies and Ventilators
- Chapter 9 Nutrition and Hydration
- Chapter 10 Legal and Professional Issues
- Chapter 11 Health and Safety
- Chapter 12 Making Ethical Decisions
- Chapter 13 Training Other Professionals
- Appendixes
- Bibliography
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.4M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Working with Dysphagia by Lizzy Marks,Deirdre Rainbow in PDF and/or ePUB format, as well as other popular books in Pedagogía & Educación general. We have over one million books available in our catalogue for you to explore.