Focusing on the latest safe and effective techniques, Endovascular Treatment of Aortic Aneurysms: Standard and Advanced Techniques provides step-by-step, comprehensive coverage of endovascular repairs of complex aneurysms of the aorta, from basic to advanced.- Explains how to perform the techniques in a step-by-step manner, using high-quality images and practical tips and tricks to optimize results.- Contains chapters devoted to the repair of leaks that may occur after a repair and the best ways to minimize radiation exposure.- Presents information in a consistent, standardized format: introduction, indications for the technique, how to perform the technique, complications and techniques for rescue, and concluding thoughts.
eBook - ePub
Endovascular Treatment of Aortic Aneurysms
Standard and Advanced Techniques
- 134 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
Endovascular Treatment of Aortic Aneurysms
Standard and Advanced Techniques
About this book
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
Topic
MedicineSubtopic
Surgery & Surgical MedicinePart I
Infrarenal Aortic Aneurysms: Standard Endovascular Aneurysm Repair
Chapter 1
The Percutaneous Approach of Endovascular Aortic Aneurysm Repair
Markus Eisenack, and Konstantinos P. Donas
Abstract
The percutaneous approach of endovascular repair of aortic aneurysms consists of use of closure devices such as the Prostar XL 10F system. The technique is safe and reproducible. The experience of the surgeon, the presence of severe calcification of the common femoral artery and scarring in the groin after previous vascular operation are significant predictors for failure of hemostasis. Contrariwise, obesity and size of the introducer system seem not to have a relevant association with suboptimal results of the endovascular percutaneous approach.
Keywords
common femoral artery; endovascular repair of aortic aneurysms; percutaneous approach; prostar system
The endovascular treatment of aortic aneurysms is based on stent-graft delivery through the common femoral artery (CFA). The procedure has evolved over the years. Since the development of the percutaneous approach in the late 1990s, several surveys have been performed and have promoted the advantages of this technique.1-4 The percutaneous approach was associated with a shorter time to ambulation and fewer complications compared with an open cutdown to the groin vessels, including a reduced risk of events such as wound infection, lymphocele, and hematomas.5
All currently available closure devices are approved for use only up to 10-French (10F) sheath sizes.6 With the introduction of the “preclose” technique, however, it was possible to close access vessels after endovascular aneurysm repair (EVAR), which requires larger-bore sheaths.7
The Prostar XL 10F device (Abbott Laboratories. Abbott Park, Illinois, USA) consists of four components (Fig. 1.1). The first two components are a hydrophilic catheter for guiding the system into the aorta and a marker lumen for identification of correct device position in the vessel (Fig. 1.2). The third component is a sheath containing four lancelike nitinol needles, which are connected to two braided sutures (Fig. 1.3). The fourth component is a rotating barrel for dissection and needle capture. The device is advanced into the artery to guide the needle trajectory through the subcutaneous tissue, with the sutures being pulled out from the inside through the arterial wall (Figs. 1.4 and 1.5).

FIG. 1.1 The Prostar XL 10F device.
Preclose Technique
After puncture of the CFA and insertion of an 8F short sheath, and with careful blunt dissection of the subcutaneous tissue down to the vessel wall with a mosquito clamp, the Prostar XL 10F is advanced and deployed. The sutures are fixed loosely with a small clamp, and a 14F sheath replaces the closure system. After deployment of the stent-graft, the sutures are tied to the vessel with a fisherman’s knot (Fig. 1.6).
To avoid major blood loss in case of a failed closure, a guidewire is left in place and maintains access to the vessel. Hemorrhage is controlled during dissection of the groin and exposure of the vessel. If oozing occurs after securing the knots, these should be held against the vessel wall with the knot pusher for several minutes, manually compressing the artery above the puncture site (Fig. 1.7).
If compression is not effective, a polytetrafluoroethylene (PTFE) felt pledget can be sewn with the four vascular sutures of the Prostar device to achieve hemostasis. The wound is closed using a topical liquid skin adhesive.

FIG. 1.2 The marker lumen of the Prostar device.
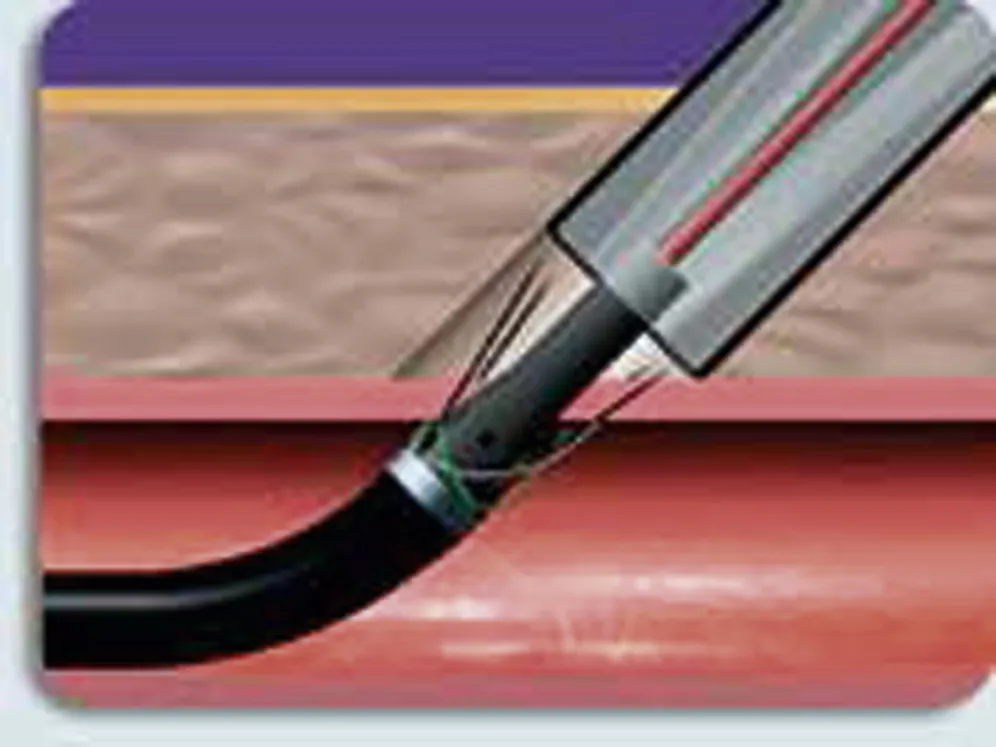
FIG. 1.3 The lancelike nitinol needles are crossed and connected to two braided sutures.

FIG. 1.4 Rotating barrel for insertion in the femoral artery. The correct position of the Prostar device in the femoral artery is confirmed by backbleeding.
Literature Review
The largest single-center series on the Prostar device was from Münster, Germany.8 Between January 2004 and December 2005, 535 consecutive patients were treated for aneurysmal disease of the aorta by endovascular means and percutaneous approach. No patient was excluded because of obesity, severe calcification of the CFA, previous interventions, or operations in the groin. The failure rate was correlated with risk factors that included obesity (body mass index [BMI] >35), extensive calcification of the CFA, previous interventions or scars in the groin, and experience of the surgeon (“experienced” defined by more than 30 closures performed with Prostar XL). Primary success was achieved in 96.1% (n = 868 groins) of all percutaneous approaches. Secondary procedures were performed in 35 cases (3.9%) to treat insufficient bleeding control (28), false aneurysm (4), or arterial thrombosis (3). In 23 cases the complications were treated by open-vessel exposure and direct suture repair. In the remaining 12 patients the failure was corrected using a PTFE pledget sutured with the Prostar sutures. The access complications were detected and treated during the first week after EVAR in all cases; no patients presented with late complications. No wound complications were recorded during the early or late period.
An assessment of factors predictive of complications identified severe calcification of the CFA (37.8%), scar in the groin (23.8%), or EVAR by a surgeon with experience of less than 30 percutaneous cases (14%). The presence of a scar in the groin also correlated with the necessity of late conversion to open femoral artery repair (P <0.001). The development of false aneurysms occurred significantly more often in scarred groins (P <0.05). Sheath size and scar in the groin also correlated with early conversion, but to a much lesser degree (respectively, P <0.05). Obesity was not a risk factor for any complication.

FIG. 1.5 The sutures are pulled through the arterial wall.

FIG. 1.6 The fisherman’s knot technique.

FIG. 1.7 A, B, Compression of the artery abo...
Table of contents
- Cover image
- Title page
- Table of Contents
- Copyright
- Dedication
- List of Contributors
- Foreword
- Preface
- Part I. Infrarenal Aortic Aneurysms: Standard Endovascular Aneurysm Repair
- Part II. Juxtarenal Aortic Aneurysms: Chimney Endovascular Technique
- Part III. Fenestrated Endografting Technique
- Part IV. Thoracoabdominal Aortic Aneurysms
- Part V. Aortic Arch and Descending Aortic Aneurysms
- Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Endovascular Treatment of Aortic Aneurysms by Konstantinos P. Donas,Giovanni Torsello,Ken Ouriel,Konstantinos Donas in PDF and/or ePUB format, as well as other popular books in Medicine & Surgery & Surgical Medicine. We have over 1.5 million books available in our catalogue for you to explore.