1. Conception
It takes just one egg and one sperm to conceive, but getting them together is not always easy. Following sex, over 250 million sperm set off on a ‘race’ to find and fertilize the egg, but only one makes it all the way to the finish to enter the egg and trigger the whole process of making your baby. These are tough odds. But this is not the beginning, because producing the sperm and eggs is the culmination of complex processes in your and your partner’s bodies, processes that must be carefully regulated by reproductive hormones (chemical messengers). So when starting to think about pregnancy perhaps the most logical starting point is to understand how your own body’s reproductive system works.
The menstrual cycle
Regular menstrual bleeding is controlled by a complex system. The brain controls the release of ‘signalling’ hormones called gonadotrophins from the pituitary gland at the base of the brain. There are two gonadotrophins: follicle-stimulating hormone (FSH) and luteinising hormone (LH).
Ovulation
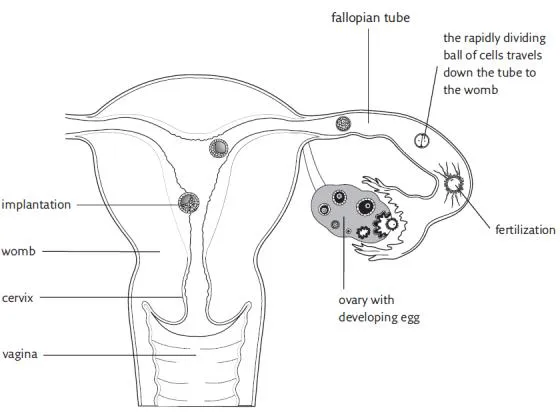
A woman is born with a lifetime’s supply of eggs. During each menstrual cycle, FSH stimulates immature eggs contained in the ovaries to develop within small fluid-filled sacs known as follicles. Initially, several eggs begin to mature but generally only one continues to develop to full maturity. This is known as the ‘dominant follicle’. Other eggs stop developing and disintegrate. When the egg is mature, the follicle it is contained within is about 2 cm (¾in) in diameter. As well as nurturing a developing egg, follicles also produce the female hormone oestrogen. When oestrogen levels are optimal and the egg is fully developed, the release of luteinising hormone (LH) occurs. This surge in the LH level triggers the release of the egg. This process is called ovulation.
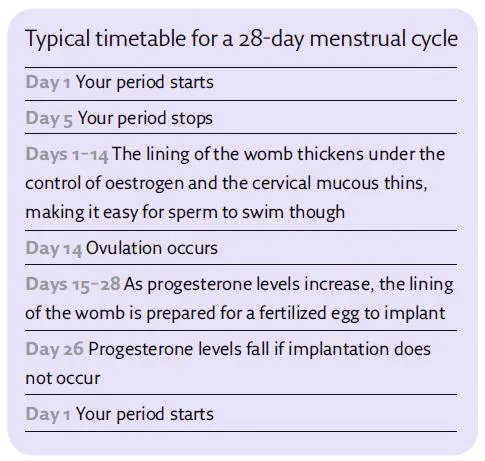
Ovulation deals with egg production. However, if this egg is fertilized, it needs to implant in the womb. So it is important for the womb to be prepared for a fertilized egg, and oestrogen has a role here too. Oestrogen stimulates the lining of the womb (the endometrium) to grow and thicken. After the egg is released from the ovary, the remains of the follicle that released the egg produces a
hormone called progesterone. (Progesterone is only made after an egg is released.) It acts on the lining of the womb by stopping its thickening at the right stage. It also improves the endometrium’s blood supply and makes it a suitable and ‘comfortable’ environment for the fertilized egg to implant.
If a fertilized egg does not implant, the production of progesterone from the ovary falls sharply. As these hormone levels fall, the blood supply to the lining of the womb is reduced and the endometrium is shed. This results in the bleeding that we know as a period. The cycle then starts over again.
Time of ovulation
As ovulation (production of a mature egg) is essential for a regular menstrual cycle, women who have a regular cycle in the normal range are usually ovulating regularly. Conversely, women who do not ovulate regularly have irregular and usually infrequent periods.
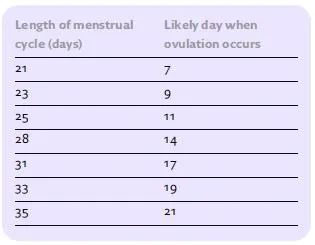
The time of ovulation depends on the length of the menstrual cycle. If a woman has a 28-day cycle, ovulation occurs at around day 14, and if she has a 21-day cycle, ovulation occurs at around day 7. The time taken to mature an egg and ovulate can vary from woman to woman. The part of the cycle during which the egg develops is called the follicular phase, as the egg develops in a small ‘follicle’ or cyst in the ovary. However, the time from ovulation to a period (if fertilization does not occur) is fixed at around 14 days. This is called the secretary phase of the cycle as the ovary makes and ‘secretes’ progesterone. Provided your cycle is regular, you will be able to estimate when you will be ovulating.
The optimum time of fertility
A woman is at her most fertile in the days around ovulation, and for a 28-day cycle this would be from days 12 to 15.
• To work out your fertile time, you need to estimate when ovulation will occur, which is usually 14 days before the first day on which your next period is due.
• For example, let’s say that your period is due to start on 24 August. Take 14 days from 24 August and this is the date around which you will ovulate. In this example, it is 10 August.
• Once an egg is released, it remains viable for around a day. Allow a day or so on either side of this for minor variations in the time of ovulation. Sperm can remain viable in the woman’s body for around two days.
• Therefore, the fertile time is estimated as being from two to three days before to two days after the estimated time of ovulation. This is the best time to try to conceive.
Some women know when they are ovulating because they feel lower abdominal pain at the time when the egg is released from the ovary. The pain is quite normal and is referred to as ‘Mittelschmerz’ (from German words for ‘middle’ and ‘pain’ – hence pain felt mid-cycle).
It’s time to conceive
Many women wonder if they need to see their doctor for a health assessment before they conceive. However, no specific check-up is usually necessary if you are healthy, have no history of miscarriage, pregnancy complications or of a long-standing medical condition.
Stopping using contraception
If you have been using a form of contraception to prevent pregnancy, depending on what method this is, the length of time it might then take you to become pregnant is affected. Barrier methods do not disturb ovulation or the menstrual cycle and you can simply stop at any time. There is no need to delay attempts to conceive provided there are no other menstrual or medical problems.
If you use an intrauterine contraceptive device, or ‘coil’, for contraception then this must be removed before you try to conceive. It is probably best to delay conception until at least the next cycle as the coil may have disturbed the lining of the womb. So, after the doctor has removed the coil, you should use another technique, such as barrier contraception, until you are ready to conceive.
If you use the oral contraceptive pill or an injectable contraceptive, your normal menstrual cycle and ovulation is disrupted. The time from stopping the pill to ovulating is extremely variable. Estimates of the time of ovulation are based on the date when the next natural (not pill-induced) period is expected, so it is impossible to estimate when ovulation will occur after stopping the pill.
If you wish to get pregnant, it is best to stop taking the pill or injectable contraceptive and wait until your normal menstrual cycle resumes before trying to conceive. As this may take about three normal menstrual periods, you might want to use a technique such as barrier contraception until your cycle has stabilized. If you become pregnant before the regular rhythm of your periods has become established, this can make it difficult to predict your delivery date based on your last period. However, a reliable estimate of the stage of the pregnancy can be obtained with an ultrasound scan to measure the size of the developing baby.
Using your body temperature to predict ovulation
Your body temperature should fall slightly before ovulation then rise quickly afterwards. It is worth noting, however, that sometimes the fall prior to ovulation is absent. The increase in temperature occurs in response to the progesterone that is produced after ovulation occurs. Progesterone levels and the body temperature remain elevated until a day or so before the next period begins. If pregnancy occurs, the temperature rise (and elevated progesterone levels) persists.
• If you want to use this technique to find out when you are ovulating, take your temperature with a thermometer in the morning before getting out of bed. Any medical thermometer that can measure in tenths of 1 °C can be used. Thermometers (including electronic ones) and temperature charts can be purchased from pharmacies.
• If you are recording an oral temperature reading, remember to check your temperature before drinking anything hot or cold to avoid getting an inaccurate reading.
• Take your temperature at the same time every day.
• Repeat for each cycle that you want to check for ovulation. If you have a regular cycle, ovulation is likely to occur at around the same time during each cycle.
The downside of using this method to check for your fertile period is that your temperature rise occurs after ovulation and by the time your temperature has risen, the egg may no longer be viable. If you have a regular menstrual cycle, however, the time of ovulation may be anticipated based on a well-recorded pattern in temperature rise. This then allows intercourse to be timed to coincide with ovulation.
Consistency of vaginal mucous
The consistency of vaginal mucous can help predict the fertile phase as the character of the discharge varies through the menstrual cycle. Just after a period, it is scant, sticky and thick. Just before the time of ovulation, when oestrogen levels are high, the amount of mucous increases and it becomes watery, stringy and clear – a bit like raw egg white.
If you collect the mucous on your finger at this time and try to stretch it between your thumb and forefinger, it elongates for several inches without breaking. After the fertile phase, the mucous again becomes thicker. Sperm can survive particularly well in the thinner ‘fertile’ mucous, which also makes it easier for the sperm to get through the cervix and into the womb. So charting the pattern of changes in your vaginal mucous can also help you work out when you are ovulating.
Ovulation prediction kit
If you want to know when you are likely to be most fertile, you could buy an ovulation prediction kit. These kits, which are available from pharmacies, measure the amount of luteinising hormone (LH) – the hormone that stimulates the release of eggs from your ovaries each month – in your urine.
The kit identifies a surge in this hormone, which precedes ovulation by around twelve hours. This can help establish the fertile days in your cycle. Ovulation prediction kits are more accurate than temperature charts and avoid the need for regular temperature assessment, but they are also more expensive.
Frequency of intercourse
However, even with temperature charts or ovulation prediction kits, it is often difficult to identify the precise time of ovulation in advance. So, from a practical perspective, you should have intercourse several times around the estimated time of ovulation. Doctors have found that having intercourse once a week makes you 50 per cent less likely to conceive than having it every couple of days. Success rates do not appear to get significantly higher if you have sex every day. Sperm survives in the woman and is capable of fertilizing an egg for around two days after intercourse, especially during her most fertile time. In addition, there is no need to restrict intercourse at other times of the month. Indeed, the best plan is to have intercourse regularly every couple of days throughout the cycle. This avoids putting pressure on you both to identify the fertile time, obliging you to make love according to the calendar rather than by desire.
Sperm production
It is the same gonadotrophins that occur in women (follicle-stimulating hormone (FSH) and luteinising hormone (LH)) that regulate sperm production in men. These hormones, or signalling molecules, are released from the man’s pituitary gland at the base of the brain.
The sperm’s journey
Follicle-stimulating hormone (FSH) stimulates the testicles to produce sperm – over 12 billion are produced each month. Luteinising hormone (LH) stimulates production of the male hormone testosterone within the testicles. Testosterone is essential for normal sperm production. After sperm are produced, they then have a long journey ahead before they are ready to fertilize an egg.
When they leave the testicles, they travel down a very fine coiled tube attached to the...