![]()
Laws That Shape Therapy Services in Educational Environments
Mary Jane K. Rapport
Mary Jane K. Rapport, PhD, PT, is Assistant Professor, Department of Special Education, College of Education, University of Florida, G315 Norman Hall, Gainesville, FL 32611.
SUMMARY. The delivery of physical therapy and occupational therapy in schools hinges, at least in part, on an accurate understanding of educational and civil rights laws that mandate services to children with disabilities in educational environments. Frequently, therapists, in addition to physicians, parents, school administrators, and teachers, have misconceptions regarding eligibility for therapy services provided at school district expense, the nature of therapy services in schools, and the frequency with which those services can and should be provided in educational environments. Most of the children who receive physical therapy, occupational therapy, or both in educational environments have disabilities that adversely affect their educational performance, and the assessments and interventions provided by therapists in educational environments are intended to be closely linked to the child’s educational program. The legal information provided in the following paper summarizes the major provisions of statutory law, federal regulations, and case law interpretation that define the perimeters established, and continually redefined, for the delivery of physical therapy and occupational therapy in schools. [Article copies available from The Haworth Document Delivery Service: 1-800-342-9678.]
INTRODUCTION
A physical therapist or occupational therapist employed by a public school district may be faced with a service delivery decision similar to that described in the following scenario: Douglas, an 8-year-old boy, was diagnosed with cerebral palsy at 4 months of age. He received numerous services as part of an early intervention program. Douglas is currently in the second grade at a local elementary school. He ambulates independently despite several observable gait deviations, and he tires more rapidly than his typically developing peers. He also has difficulty performing some of the more complex activities on the playground (e.g., climbing bars and tether ball). As a result of limited use of his left arm, Douglas requires modifications for many of the projects in art class. He is able to complete all assigned written seat work in academic subjects with either additional time or the use of a computer for word-processing. Should Douglas receive physical therapy, occupational therapy, or both at school district expense?
Several other pieces of information are necessary to answer this question. In Douglas’ case, it is possible that the local school district may not be financially responsible for providing therapy for Douglas. This outcome, however, does not preclude the fact that Douglas might benefit from continued therapy provided in the community (i.e., therapy that is financed by resources other than the school district) to work on goals that are related to, but not directly assimilated into, his educational program. For example, Douglas may continue to work with a community-based therapist on skills that will eventually lead to improved or independent performance on various pieces of playground equipment. Although the ability to recreate independently may be an educationally-related goal for some children with disabilities, the ability to independently negotiate all pieces of playground equipment may not be a goal of educational relevance for Douglas. Age is but one factor that might be considered by a child’s multidisciplinary team in determining the importance of providing therapy services related to the use of playground equipment. Conversely, the team may identify areas in which Douglas’ disability does adversely affect his educational performance (e.g., high level of fatigue related to energy expenditure required to walk or limited use of his left arm for classroom activities) and may recommend therapeutic intervention as related services to be provided at school district expense. If Douglas’ multidisciplinary team decides that he needs therapy to accomplish his educational goals, whatever they are, or to have access to or be maintained in the least restrictive educational environment, then the school district needs to provide it.
Understanding the role of occupational therapy and physical therapy in the educational environment has always been important, but in light of the current shortage of therapists and the mounting financial concerns of school districts nationwide, it has become ever more critical that therapy services be provided in accordance with both best practice and the parameters established by federal and state law. Appropriate delivery of therapy services in schools hinges, at least in part, on an accurate understanding of the laws that mandate related services for children with disabilities in educational environments.
STATUTES, REGULATIONS, AND CASE LAW
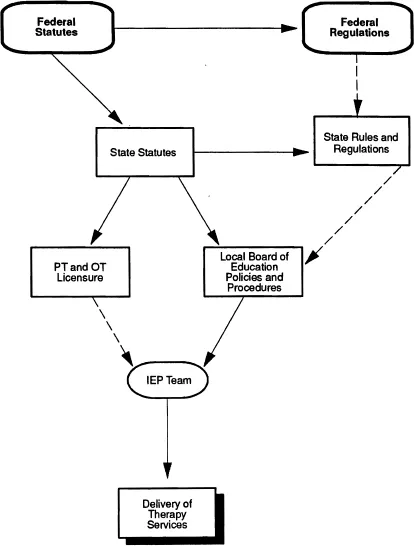
The provision of therapy services has been included in federal education statutes1 and described briefly in accompanying federal regulations.2 Statutes are legislative acts and regulations are the guidelines established by governmental agencies to carry out the laws or statutes. State statutes and regulations, as well as local board policies, provide additional guidelines for the delivery of therapy services in the educational environment. The federal component of this legal system provides the framework within which other jurisdictions must comply. As a result, neither state statutes nor local board policy may establish standards of service delivery below those set by federal statutes and regulations governing such practices. Figure 1 provides a visual representation of the legislative impact on the delivery of therapy services.
Statutes, the formal legislative component of the law, are developed and approved when sufficient case law and changing societal trends cause legislators to accept a “call” for action. It is through such legislative processes that updated federal and state statutes since the mid 1970s have included physical therapy and occupational therapy as related services to be provided at no cost to parents within the educational programs of children with disabilities. Federal regulations provide many general and specific guidelines for the delivery of services to children with disabilities, but state and local laws, board policies, and procedures also are important in determining eligibility and developing guidelines for the delivery of services. Case law, or judge-made law, provides additional information and interpretation of existing statutes and regulations when two parties have disagreed on the legal interpretation of a rule, regulation, or policy and have brought the disagreement before the courts. When considering the case study of Douglas described above, the provision of therapy services would be based not only on federal and state statutes (laws) and regulations (rules and procedures) but also on local board policy and perhaps on interpretation from a state hearing officer in response to due process or an otherwise judicially-based decision.
The legislative “hierarchy” represented in Figure 1 depicts federal statutes as having precedence over state and local governments and agencies. This hierarchical structure also exists within the judicial system, whereby decisions conferred by the United States Supreme Court super-sede all decisions made in any lower courts of law (e.g., state supreme courts, federal district courts, and federal appellate courts).
FIGURE 1. Legislative Impact on the Delivery of School-Based Therapy Services
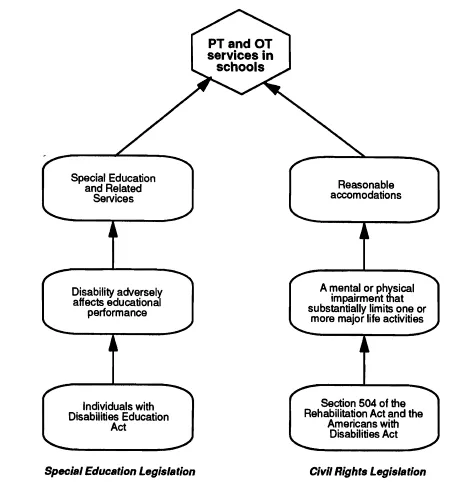
Several federal laws contain provisions for delivery of physical therapy and occupational therapy in schools. The most important of these is the Individuals with Disabilities Education Act (IDEA)1 which requires compliance by all federal financial recipients in the provision of special education and related services to children who have disabilities that adversely affect educational performance. Section 504 of the Rehabilitation Act (RA)3 and the Americans with Disabilities Act (ADA)4 represent other important civil rights statutes that also affect the delivery of therapy services to children with disabilities in schools, although to a lesser degree than IDEA. These statutes, and their impact on therapy services in schools, will be described later. Figure 2 depicts how children with disabilities may be eligible for physical and/or occupational therapy services in schools according to the federal statutory definitions provided under the RA (Section 504), the ADA, and IDEA.
THE INDIVIDUALS WITH DISABILITIES EDUCATION ACT
Physical therapy and occupational therapy are included among the long list of related services in the Individuals with Disabilities Education Act of 1990 (formerly the Education of the Handicapped Act) that may be required “to assist a child with a disability to benefit from special education.”5 IDEA is the single most influential piece of federal legislation associated with the delivery of therapeutic intervention within educational environments. Two parts of the statute contain information specific to the delivery of physical therapy and occupational therapy: Part B6 and Part H.7 Part B currently applies to children ages 3 through 21 who require specially designed instruction to meet their unique needs.
Part H responds to the needs of children birth through age 2 (i.e., up to 36 months of age or the child’s third birthday) who have an identified disability and who are experiencing, or have a high probability of experiencing, developmental delay and to their families.8 Children who are at-risk for substantial developmental delay without early intervention are also included under Part H at the state’s discretion.9 Federal legislation mandating services to very young children (Title I: birth through age 2, and Title II: ages 3 through 5) with disabilities, and those who are at-risk, was implemented with the enactment of Public Law 99–457, the 1986 Amendments to the Education of the Handicapped Act (EHA).10 Physical therapy and occupational therapy are provided as related services under Part B5 and as early intervention services under Part H.11
FIGURE 2. Statutory Eligibility for School-Based Therapy Services
Part B has a far greater impact than Part H on the delivery of therapy services in schools simply by virtue of the age range of children protected under this statute (ages 3 through 21), but Part H does provide services for young children in educationally-related, center-based locations when appropriate. Part H programs are under the auspices of the Department of Education in those states where that state department has been designated as the lead agency for early intervention services. This paper will focus primarily on Part B in Table 1, although the regulations for several relevant sections of Part H can be found in Table 2 and compared with the similar sections from Part B in Table 1. The tables provide definitions for several important terms used within IDEA pertaining to the delivery of special education and related services.
IDEA, like many other federal statutes, requires periodic reauthorization to assure continued appropriations and provide opportunities for modifications, additions, or deletions in the procedural and substantive components of the existing statute. As the reauthorization process that began last year (1994) conti...