![]()
Section 1
Epidemiology
1. Worldwide Epidemic of Obesity
2. Social and Ethnic Determinants of Obesity
3. Genetic and Molecular Basis of Obesity
4. The Psychological Basis of Obesity
5. Obesity in Adolescence
![]()
1
Worldwide Epidemic of Obesity
Rohana N. Haththotuwa1, Chandrika N. Wijeyaratne2 and Upul Senarath3
1Ninewells Care Mother and Baby Hospital, Colombo, Sri Lanka
2Department of Obstetrics and Gynaecology, Faculty of Medicine, University of Colombo, Colombo, Sri Lanka
3Department of Community Medicine, Faculty of Medicine, University of Colombo, Colombo, Sri Lanka
Introduction
Obesity has reached epidemic proportions globally and has more than doubled worldwide since 1980. According to the estimates by the World Health Organization (WHO) in 2008, more than 1.5 billion adults were overweight, and of those, over 200 million men and nearly 300 million women were obese [1]. WHO in 1997 formally recognised obesity as a global epidemic by designating obesity as a major public health problem [2]. As obesity is becoming an epidemic, concern over its significant health and economic consequences has also grown. The problem of obesity is a major contributor to the global burden of chronic disease and disability. Often coexisting with undernutrition in developing countries, obesity is a complex condition, with serious social and psychological implications that affects virtually all ages and socio-economic groups [3].
Although overweight and obesity were once perceived as a sign of affluence, it has been increasingly recognised as an important health risk that affects men and women, particularly in low- and lower-middle income countries. This has been largely due to the effects of globalisation and rapid and unplanned urbanisation leading to major behavioural changes in the world’s populations. Obesity is now recognised as a health risk that is not limited to affluence but affecting the lower socio-economic strata, and among the poorer groups particularly women. The troublesome aspect of this problem is the parallel emergence of childhood and adolescent obesity in many parts of the world. The latter brings into focus the role of obesity in women of reproductive years, which is also linked to obesity in their offspring. Although the main impact of obesity is its cardiometabolic risks that lead to greater occurrence of cardiovascular morbidity and mortality that has reached a crisis point on the socio-economic status of the affected populations, it has also been identified as a major contributory factor for infertility among both men and women.
This chapter collates the available epidemiological data on overweight and obesity affecting women the world over. The epidemiological features of obesity, including global prevalence, secular trends and associated factors, and burden of illness related to obesity are addressed.
Definitions of Overweight and Obesity
Obesity is defined as an abnormal or extensive fat accumulation that may impair the health of an individual. Because fat is stored throughout the body, it cannot be measured directly. Body weight itself cannot provide an indication of fat stores. Instead, other measurements including body mass index (BMI), waist circumference, waist/hip ratio, skinfold thickness and bio-impedance are used to assess obesity and overweight.
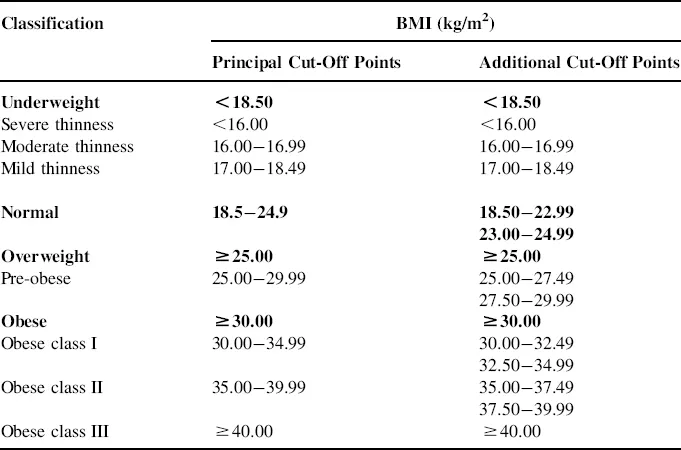
The prevalence of overweight and obesity is commonly assessed by using BMI, defined as the weight in kilograms divided by the square of the height in metres (kg/m2). BMI is classified according to the criteria laid by the National Institute of Health in the United States and is recommended by WHO. In general, BMI less than 18.5 kg/m2 is considered underweight, 18.5–24.9 kg/m2 is normal, 25 kg/m2 or greater is overweight and 30 kg/m2 or greater is obese [4]. Table 1.1 summarises the details of the international classification of adult underweight, overweight and obesity according to BMI. The WHO definition of obesity includes central obesity as waist circumference greater than 102 cm in men and 88 cm in women [2].
Table 1.1 The International Classification of Adult Underweight, Overweight and Obesity According to BMI
*Values in bold represent underweight, normal, overweight and obese according to BMI
Source: Ref. [4].
There is less clarity whether these criteria are applicable for all racial groups due to ethnic variation in body composition and for children and the older groups who have a decline in muscle mass. Nevertheless, the international convention based on the two major WHO technical consultations in 1995 and 2000 endorsed the use of a common BMI scheme for adults irrespective of sex or age [2].
Manifestation of the consequences of insulin resistance, particularly in Asian populations, due to abdominal visceral fat with lower values of BMI warrants due attention to be paid to central obesity. Abdominal fat is closely linked with a greater metabolic risk of diabetes, hypertension, ischaemic heart disease, strokes and gall bladder disease; these diseases have an ethnic variation possibly due to socio-cultural influences [5–8]. Therefore, measurement of waist circumference must be included in the overall assessment of an individual’s health-risk categorisation of overweight and obesity. The recommended measure of waist circumference is at the level of the mid-point between the 12th rib and upper margin of the iliac crest when standing (determined from the posterior aspect) in mid inspiration using a non-expansible tape measure.
It was proposed to lower cut-off points for BMI and waist circumference for use in Asian communities [9]. Furthermore, evidence has emerged that Afro-Caribbean, Hispanic Americans, Asian Indians, Chinese and Latin Americans have a greater risk of accumulation of excess adipose tissue in the abdominal viscera than white Caucasians [10]. The basis for this recommendation of using differing cut-offs for ethnic groups was based on the observation that they consistently manifested metabolic problems at a lower BMI [11–14]. A new analysis has also proposed different values for the Chinese [15]. Therefore, the current clinical consensuses are to identify obesity at a lower BMI in ethnic groups originating from Asia in particular and also to pay due attention to waist circumference.
The Extent of the Problem
The estimates made by the WHO indicate that the problem of obesity extends globally. In 2008, 1.5 billion adults, 20 and older, were overweight. Of those, over 200 million men and nearly 300 million women were obese [1]. According to the global database on BMI compiled by the WHO, the prevalence of obesity varied widely across countries. The obesity levels (BMI≥30 kg/m2) range from below 5% collectively in China, Japan, India, Indonesia and certain African nations to over 75% in Samoa and Nauru [4]. But even in relatively low-prevalence countries like China and Japan, rates were almost 20% in some cities [3,16]. The most recent available data reveal that the prevalence of obesity in adults in the United States is 33.9% compared to 23.1% in Canada, 22.7% in the United Kingdom, 16.9% in France and 16.4% in Australia [4]. However, it is important to note that the data presented might not be directly comparable since they vary in terms of sampling procedures, age ranges and the year of data collection. The incidence of obesity reported across different countries should be interpreted with great caution as there are different age structures in the populations, measurement techniques used are not comparable and surveys may not be population-based.
Childhood obesity is already an epidemic in some countries and is on the rise in others. Approximately, 22 million children under 5 years of age are estimated to be overweight worldwide. In the United States, the number of overweight children has doubled and the number of overweight adolescents has trebled since 1980. The prevalence of obese children aged 6–11 years has more than doubled since the 1960s. Obesity prevalence in adolescents aged 12–17 years has increased dramatically from 5% to 13% in boys and from 5% to 9% in girls between 1966–1970 and 1988–1991 in the United States. The problem is global and increasingly extends into the developing world; for example, the prevalence of obesity in 5- to 12-year-old children in Thailand rose from 12.2% to 15.6% in just 2 years [3]. Sedentary lifestyle and rapidly changing dietary practices have led to increasing prevalence of obesity in children aged 5–19 years in developing countries [17,18]. A recent review found huge variation in the prevalence of childhood obesity: 41.8% in Mexico, 22.1% in Brazil, 22.0% in India and 19.3% in Argentina. Moreover, secular trends indicate increasing prevalence rates in these countries: 4.1–13.9% in Brazil during 1974–1997, 12.2–15.6% in Thailand during 1991–1993 and 9.8–11.7% in India during 2006–2009 [17].
In Mexico, the prevalence of overweight and obesity is 16.7% in preschool children, 26.2% in school children and 30.9% in adolescents. For adults, the prevalence of overweight and obesity is 39.7% and 29.9% respectively [19].
Temporal Trends
Worldwide, the prevalence of obesity has increased dramatically during the last three decades. In the United States, the prevalence of excess weight is increasing rapidly across the country, and almost 65% of the adult population was overweight or obese by the year 2000 [20]. Compared with the period 1976–1980, the prevalence of overweight (BMI≥25 kg/m2) had increased by 40% (from 46.0% to 64.5%) and the prevalence of obesity (BMI≥30 kg/m2) had risen by 110% (from 14.5% to 30.5%) by 1999–2000 [20,21]. An alarming increase in weight among the youths in the United States has also been observed. More than 10% aged 2–5 years and 15% aged 6–19 year are overweight (BMI≥95th percentile for age and gender) [22]. This represents a near-doubling of overweight children and a near-tripling of overweight adolescents over the last two decades. Although some segments of the population are more likely to be overweight or obese than others, people of all ages, socio-economic levels, ethnicities, races and geographic areas are experiencing a substantial increase in weight [23].
International data indicate that the rising trend is not only confined to the United States and other developed countries but it is in fact a global health problem as the prevalence of obesity is also rising in less-affluent countries as well. The prevalence of obesity increased dramatically during the last decades [2,4,24–26] in the developed countries as well a...