![]()
1 Introduction
Integrative Treatment of Complex Trauma for Children (ITCT-C) is an
evidence-based, component-driven model that integrates a variety of theoretical
and clinical approaches to the treatment of complex trauma in children.
Development and evaluation of this therapy was supported by the Substance Abuse
Mental Health Services Administration, through its funding of the Miller
Children’s Abuse and Violence Intervention Center (MCAVIC) from 2001–2005 and
the MCAVIC-University of Southern California (MCAVIC-USC) Child and Adolescent
Trauma Program from 2005–2009.
Although ITCT-C was originally designed for the treatment of multiply traumatized
children aged 8 to 12 years, this book also includes interventions that can be
adapted for children ages 5 to 7 years. There is also an adolescent version of
ITCT, Integrative Treatment of Complex Trauma for Adolescents (ITCT-A), for
youth aged 12–21, which is described in its associated treatment guide (Briere
& Lanktree, 2013) and a separate volume (Briere & Lanktree,
2012).
ITCT-C has been empirically evaluated (Lanktree et al.,
2012) and has been expanded considerably since the original treatment
guide was released in 2008. This book incorporates extensive feedback from
clinicians and workshop participants over the past five years, to whom the
authors owe a debt of gratitude.
Because this is a comprehensive treatment model, its effectiveness is enhanced by
the therapist’s knowledge, skill, and openness to the client, and his or her
actual enjoyment of the therapy process. Although specific interventions and
activities are described, this is not a how-to manual, nor is it based on a “one-size-fits-all” approach. ITCT-C is
designed to inspire therapists to approach the treatment of complex trauma in
children from various perspectives. It offers a range of treatment components
that are applied based on the results of ongoing assessment (using the
Assessment-Treatment Flowchart for Children), and allowing for adaptations based
on the client’s age, developmental level, level and type of symptomatology, and
cultural/ethnic background.
Unlike some other approaches for traumatized children, wherein treatment is
limited to 12 to 16 weeks or less, ITCT-C is extendable to whatever period of
time is most helpful in reducing the child’s trauma-related difficulties. In
many cases, the effects of complex trauma are unlikely to remit in the span of
several months—especially when the client suffers from a number of different
symptoms and problems, there is a risk of further victimization, other
environmental stressors are common, and attachment issues are prominent. In such
cases, ITCT-C may easily require treatment periods which extend to 6 months or
longer. Nevertheless, ITCT-C has been adapted to settings where shorter-term
treatment interventions are required, for example, where there are funding
constraints or where short-term treatment is the only option (e.g., drop-in
clinics, homeless shelters, residential treatment facilities).
ITCT-C is relationally based, incorporating tenets of complex trauma theory
(e.g., Ford & Courtois, 2013), attachment theory (e.g., Bowlby, 1988),
cognitive behavioral approaches (e.g., Cohen, Mannarino,
& Deblinger, 2006), and the Self Trauma Model (e.g., Briere
& Scott, 2014). Because it is oriented toward the treatment of
complex trauma, it can be used to address the effects of a wide range of adverse
experiences, including child abuse and neglect, traumatic bereavement, assaults
by peers, community violence, witnessing parental domestic violence, parental
substance abuse, and trauma associated with severe illness or injury. It also
includes a focus on the various impacts of insecure caretaker-child attachment
relationships as they add to, compound, or intensify the psychological effects
of traumatic experiences.
There are a variety of treatment components within this model, for example,
affect regulation training, titrated exposure to traumatic memories, cognitive
and emotional processing, and attachment/relational interventions, all of which
are differentially utilized according to each child’s specific problems or
issues. As compared to interventions for adolescents (e.g., ITCT-A), ITCT-C has
a stronger emphasis on symbolic and expressive play approaches, the option of
shorter individual therapy sessions for the child, greater emphasis on
collateral and family sessions to facilitate appropriate caretaker support and
parenting skills, and more of a focus on insecure attachment as it plays out in
child-caretaker relationships.
In addition to individual therapy, ITCT-C can involve collateral, family, and
group therapy. Weekly collateral sessions with primary caretakers are integral to the model. Because of the
critical role of caretakers in the younger child’s life, ITCT-C may also
facilitate trauma recovery for the primary caretaker(s) in their own individual
therapy, group sessions, or collateral treatment. In such cases, treatment may
include the caretaker’s processing of traumatic experiences—both their own as
well as the impacts of the child’s victimization—so that they can become more
attuned to the child’s needs and develop a more secure caretaker-child bond.
This approach also includes optional parent education classes, which are
provided for caretakers struggling with parenting issues, as well as group
sessions for caretakers involving trauma-related psychoeducation, trauma
processing with peer support, and exploration of relationships and family
systems.
As described in Chapter 17 and elsewhere, ITCT-C has been
adapted for children in urban school environments, including “alternative” or
“storefront” settings for high-risk students. The primary modality in such
contexts is group therapy, with individual crisis counseling and shorter-term
therapy sessions provided when needed. Teachers, school counselors, and social
workers also receive consultations, training, and support. Parents are engaged
whenever possible, but school-based interventions may be limited by less access
to parents due to the schools’ hours of operations, as well as caretakers’ work
demands, transportation problems, and, on occasion, discomfort with going to
school sites.
ITCT-C particularly targets economically disadvantaged and culturally diverse
children, many of whom are coping with additional stressors associated with
poverty, unsafe communities, and social marginalization. Frequently, ITCT-C
clients are dealing with immigration issues, acculturation challenges,
separation from primary caretakers—some of whom may remain in their country of
origin, and attachment/relationship problems associated with being reunited with
family members after a period of separation. At the same time, however, ITCT-C
is also used in settings with clients who may not be as economically or socially
disadvantaged, and who may not be facing the same degree of external
stressors.
Importantly, the client’s history of insecure attachment relationships and
negative relational schema is addressed in his or her individual ITCT-C
sessions. The therapeutic relationship invariably triggers trauma-related
thoughts, feelings, and memories in the child, which, in the context of safety
and security, can be processed and counterconditioned.
Empirical Support for ITCT
A treatment outcome study (Lanktree et al., 2012) conducted over a
period of several years evaluated the effectiveness of ITCT (both ITCT-C and
ITCT-A) in reducing trauma-related
symptomatology in a culturally diverse, largely inner-city sample of 151
children and adolescents. Most children were seen in a clinic environment,
although some attended the school-based adaptation. In most cases,
caretakers attended collateral therapy as described in Chapter
15.
A significant majority of these children had experienced multiple types of
trauma, typically some combination of childhood sexual or physical abuse,
psychological maltreatment, emotional neglect, family violence, loss of a
loved one, community violence, and parental substance abuse, often
compounded by caretaker-child attachment issues. In addition, some were
referred by local hospitals and clinics following a traumatic medical
condition (e.g., HIV/AIDS), injury (e.g., gunshot wound), or invasive
medical procedure (e.g., amputation).
Although this study did not include a control group, clients’ scores on the
Anxiety, Depression, Anger, Posttraumatic Stress, Dissociation, and
Sexual Concerns scales of the Trauma Symptom Checklist for Children
(TSCC; Briere, 1996) decreased an average of 41%
(p < .001) over an average of 6 to 7 months. There were no differences in
treatment effectiveness in relation to gender, number of traumas, ethnicity,
or whether the client received ITCT-C or ITCT-A. However, longer-term
treatment was associated with greater symptom reduction, as per other
research in this area (e.g., Lanktree & Briere, 1995).
Structure of This Book
This treatment guide defines and describes complex trauma and its effects,
followed by a discussion of the ITCT-C approach to psychological assessment,
including the Assessment-Treatment Flowchart for Children (ATF-C). The
reader is then introduced to the ITCT-C Problems-to-Components Grid (PCG-C),
which assists the clinician in applying the results of the ATF-C to create a
specific treatment plan for the child. Remaining chapters then present the
treatment components that, as identified by the PCG-C, can be used to
implement a customized approach to the child’s specific needs. These
components are: Relationship Building and Support, Safety Interventions,
Psychoeducation, Advocacy and Systems Interventions, Distress Reduction
and Affect Regulation Training, Facilitating Positive Identity,
Cognitive and Emotional Processing, Relational/Attachment Processing,
Interventions with Caretakers, Family Therapy, and School-Based
Adaptations. Finally, a chapter on ITCT-C supervision and therapist
self-care is presented, followed by appendices containing ITCT-C tools and
worksheets.
![]()
2 Effects of Complex Trauma in Children
One of the insights that has emerged as clinicians and researchers study and treat complex trauma effects is, in fact, the complexity of many maltreatment-related responses and the conditions under which they are likely to occur. This chapter reviews the meaning of complex trauma, its primary effects, and variables that complicate or intensify the clinical picture for children.
Complex Posttraumatic Events
Complex trauma can be defined as a combination of early and later-onset, sometimes invasive adverse events, usually of an ongoing, interpersonal nature. In most cases, it includes repetitive childhood sexual, physical, and/or psychological abuse, often in the context of other family violence, concomitant emotional neglect, and harmful or marginalizing social environments. Some children also may have experienced medical trauma (e.g., chronic serious illness or serious physical injury) and/or traumatic loss.
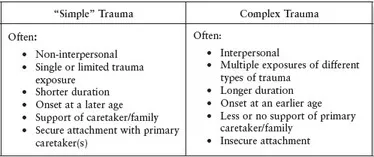
Differences between “simple” or single incident traumas and more complex scenarios are presented below:
Effects of Complex Trauma
As noted by Cook et al. (2005), “children exposed to complex trauma often experience lifelong problems that place them at risk for additional trauma exposure and cumulative impairment … in childhood, adolescence and adulthood.” The impacts of complex trauma typically extend beyond posttraumatic stress and often include attachment, self-capacity, dissociative, somatic, cognitive, and/or behavioral domains (Briere & Spinazzola, 2009; Cook et al., 2005; Hodges et al., 2013). In such cases, although children may be diagnosed with PTSD, major depression, and/or some form of anxiety disorder, these diagnoses generally capture only a limited aspect of the traumatized child’s symptoms, impairments, and behaviors.
A review of the literature suggests that exposure to complex trauma in childhood is associated with the following:
- Anxiety and depression, including panic attacks, free-floating anxiety, and phobias, as well as sad mood and major depression
- Cognitive distortions, such as low self-esteem, extreme helplessness, hopelessness, and potential overestimation of the amount of danger in the environment
- Insecure attachment, sometimes involving disorganized attachment, reactive attachment disorder, or a disinhibited social engagement disorder, as well as, more generally, problems associated with close relationships, including excessive clinging or neediness, separation anxiety, or, alternatively, avoidance of attachments to parents or significant others
- Posttraumatic stress, including reexperiencing symptoms (e.g., nightmares and posttraumatic play), avoidance behaviors (e.g., avoiding people or situations reminiscent of the trauma), hyperarousal/reactivity (e.g., hyperactivity, attention and concentration problems, aggression), numbing, and negative cognitions and mood
- Dissociation, including depersonalization, derealization, and disengagement
- Identity disturbance, including attachment-related problems in self- and boundary awareness
- Affect dysregulation, involving a relative inability to tolerate or control emotions and painful internal states, often leading to “externalized” behaviors
- Interpersonal problems, ranging from difficulties in forming positive, stable friendships to excessive distrust of others
- Self-injury, generally involving, in children, intentional behavior such as head banging, biting, cutting, or hitting self
- Sexual disturbance, such as preoccupation with sexual thoughts or feelings, or sexualized behavior, such as inappropriate sex play or involving others in unwanted sexual activity
- Enuresis and encopresis, involving problems with bladder or bowel control
- Somatization, involving excessive preoccupations with bodily dysfunction and/or multiple bodily complaints
- School-related difficulties, primarily learning disabilities and poor academic performance
- Social withdrawal, such as avoiding social interactions or friendships, or self-isolation
- Conduct disturbance, including truancy, aggression, stealing, or excessive rule-breaking
- Suicidality, which, although less common in younger children, may involve thoughts of killing oneself or actual suicidal behavior
The reader is referred to the following reviews for more information on trauma-symptom relationships in children: Briere & Spinazzola (2009); Cook et al. (2005); Ford & Courtois (2013); Meyers (2010); Nader (2007); the National Child Traumatic Stress Network (n.d.); Putnam (2003); and van der Kolk (2005).
Phenomena That May Intensify, Compound, or Complicate Trauma Effects
The list presented above may appear to suggest that the abuse-outcome relationship, although wide-ranging, is relatively straightforward. However, it is almost always true that other events, processes, and conditions intensify or complicate the effects of childhood trauma or maltreatment. Among these moderators of trauma impacts are the following:
Poverty and social marginalization. Social and economic deprivation, as well as racial, ethnic, or gender-based discrimination not only produce their own negative effects on children, they increase the likelihood of trauma exposure and often intensify and complicate the effects of such victimization (Collins et al., 2010). Children who are socially or economically marginalized may not be able to play or move about their neighborhoods freely without threat of violence. The increased stress of being constantly vigilant to danger, including from gang-related activity, combined with parental struggles to support their families financially, and the child’s reduced access to health and mental health services, can contribute further to the impacts of trauma or maltreatment.
Intensity, invasiveness, and complexity of maltreatment. Bodily violation, especially in sexual abuse, can especially result in symptomatology (Berliner, 2011; Collins et al., 2010). At the same time, it is rarely true that such acts occur in isolation. In the case of sexual abuse, for example, invasiveness is frequently accompanied by repeated and ch...