
eBook - ePub
Atlas of Diagnostic Endoscopy, 3E
Mohammad Ibrarullah
This is a test
- 186 pages
- English
- ePUB (adapté aux mobiles)
- Disponible sur iOS et Android
eBook - ePub
Atlas of Diagnostic Endoscopy, 3E
Mohammad Ibrarullah
Détails du livre
Aperçu du livre
Table des matières
Citations
À propos de ce livre
This book is a compilation of endoscopic images of the upper gastrointestinal tract. The 3rd edition is enriched with high-resolution digital images highlighting the classification and staging of endoscopically relevant diseases. Serial documentation of diseases and procedures like corrosive injury, variceal obliteration, peptic ulcer etc. provides a complete, informative and interesting perspective. Rare conditions like Dieulafoy's disease and Gastric antral vascular ectasia (GAVE) have been extensively discussed along with common diseases of the GI tract. This book outlines the technique and interpretation of endoscopic images proving to be a helpful guide to endoscopy practitioners.
Key Features
-
- Explores various GI tract diseases through coloured, high resolution clinical photographs.
-
- Serves as a useful reckoner for trainee endoscopists and practitioners pursuing gastroenterology or gastrointestinal endoscopy.
-
- The text is updated with tables, flowcharts, classifications and international treatment guidelines.
Foire aux questions
Comment puis-je résilier mon abonnement ?
Il vous suffit de vous rendre dans la section compte dans paramètres et de cliquer sur « Résilier l’abonnement ». C’est aussi simple que cela ! Une fois que vous aurez résilié votre abonnement, il restera actif pour le reste de la période pour laquelle vous avez payé. Découvrez-en plus ici.
Puis-je / comment puis-je télécharger des livres ?
Pour le moment, tous nos livres en format ePub adaptés aux mobiles peuvent être téléchargés via l’application. La plupart de nos PDF sont également disponibles en téléchargement et les autres seront téléchargeables très prochainement. Découvrez-en plus ici.
Quelle est la différence entre les formules tarifaires ?
Les deux abonnements vous donnent un accès complet à la bibliothèque et à toutes les fonctionnalités de Perlego. Les seules différences sont les tarifs ainsi que la période d’abonnement : avec l’abonnement annuel, vous économiserez environ 30 % par rapport à 12 mois d’abonnement mensuel.
Qu’est-ce que Perlego ?
Nous sommes un service d’abonnement à des ouvrages universitaires en ligne, où vous pouvez accéder à toute une bibliothèque pour un prix inférieur à celui d’un seul livre par mois. Avec plus d’un million de livres sur plus de 1 000 sujets, nous avons ce qu’il vous faut ! Découvrez-en plus ici.
Prenez-vous en charge la synthèse vocale ?
Recherchez le symbole Écouter sur votre prochain livre pour voir si vous pouvez l’écouter. L’outil Écouter lit le texte à haute voix pour vous, en surlignant le passage qui est en cours de lecture. Vous pouvez le mettre sur pause, l’accélérer ou le ralentir. Découvrez-en plus ici.
Est-ce que Atlas of Diagnostic Endoscopy, 3E est un PDF/ePUB en ligne ?
Oui, vous pouvez accéder à Atlas of Diagnostic Endoscopy, 3E par Mohammad Ibrarullah en format PDF et/ou ePUB ainsi qu’à d’autres livres populaires dans Medicina et Teoría, práctica y referencia médicas. Nous disposons de plus d’un million d’ouvrages à découvrir dans notre catalogue.
Informations
1
Techniques of UGI endoscopy and normal anatomy
Preparation for endoscopy
Informed consent and counseling: The patient should be clearly informed about the procedure and the likely discomfort he may experience. It should be explained that his cooperation will make the procedure easier and quicker.
Overnight fasting: Routine endoscopy is usually performed in the morning hours after overnight fasting. Coating agents like antacids or colored medications should be clearly withheld. In case of obstructed stomach, prior nasogastric intubation and lavage should be performed to clear the gastric residue.
Sedation and anesthesia: For routine UGI endoscopy, we use only topical pharyngeal anesthetics such as lignocaine viscous or spray. Sedation, in the form of intravenous Midazolam, is occasionally used in children. For therapeutic endoscopy, such as foreign body removal, stent placement etc., it is our practice to use intravenous propofol anesthesia with or without endotracheal intubation.
Endotracheal intubation and monitoring: Endoscopy in a comatose or irritable patient is fraught with the risk of aspiration, hypoxia and “bite” damage to the endoscope. It is our practice to use prior endotracheal intubation and also monitor the vital parameters during the procedure.
Instrument check: Prior to endoscopy, it is good practice to check the instrument, including the light source, suction channel, airflow and display panel for any malfunction.
Position of the patient: Diagnostic endoscopy is always performed in the left lateral position. Occasionally, in a patient with upper GI bleeding, it may be necessary to examine the patient in the right lateral position. This is to displace the fundal blood pool that may obscure the bleeding lesion.
Antibiotic prophylaxis: Antibiotic prophylaxis is not indicated for diagnostic endoscopy. Current recommendations by the American Society for Gastrointestinal Endoscopy (ASGE) exclude even conditions such as valvular heart disease, prosthetic valves, synthetic vascular graft and prosthetic joints from the ambit of antibiotic prophylaxis. The few indications for antibiotic prophylaxis are therapeutic endoscopy for cirrhosis with acute variceal bleeding, cyst drainage and in patients with established GI tract infection who have the above listed cardiovascular status.
The mouth guard is held between the teeth. It is further supported by the index and middle finger of the endoscopy assistant. Alternatively, an elastic band attached to the mouth guard can be used to keep it steady.
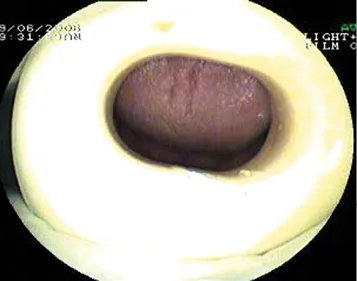
Figure 1.1 The mouth guard.
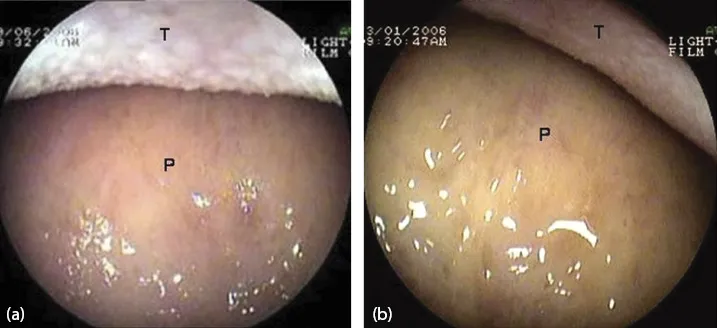
Figure 1.2 View as the endoscope enters the oral cavity. (a, b) Dorsum of the tongue (T) and hard palate (P).
The tip of the endoscope is slightly bent to fit the contour of the tongue. It is gently advanced over the base of the tongue towards the pharynx.
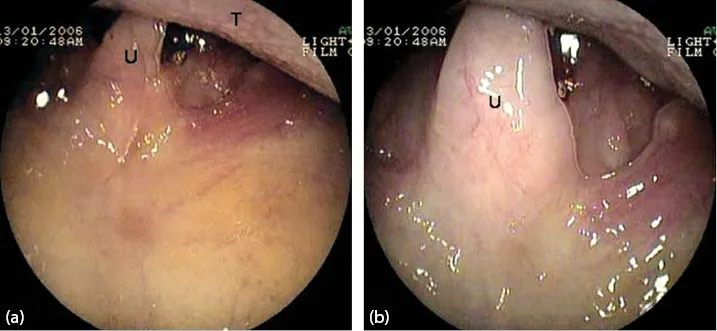
Figure 1.3 (a, b) Uvula (U) and the base of the tongue (T).
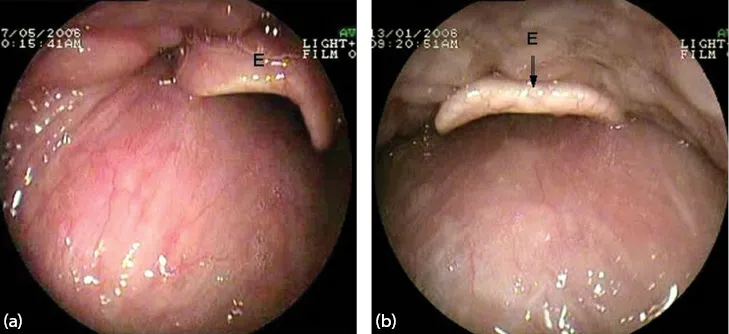
Figure 1.4 (a, b) Epiglottis (E).
The epiglottis (E) is seen as the pharynx is entered.
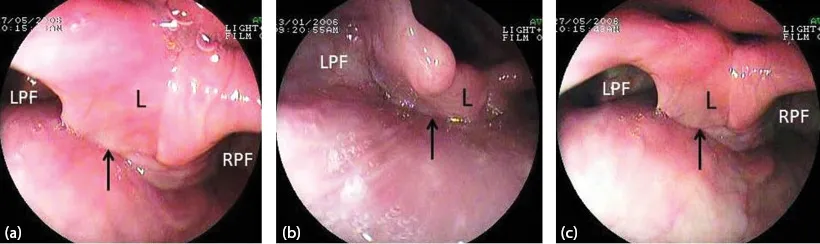
Figure 1.5 (a–c) The laryngo-pharynx. Larynx (L) and both pyriform fossae (RPF, LPF). The arrow points to the esophageal inlet.
As the scope passes below the epiglottis, the larynx and both pyrifo...