eBook - ePub
Thoracic Imaging
Illustrated Clinical Cases, Second Edition
Sue Copley, David Hansell, Jeffrey Kanne
This is a test
- 212 pages
- English
- ePUB (adapté aux mobiles)
- Disponible sur iOS et Android
eBook - ePub
Thoracic Imaging
Illustrated Clinical Cases, Second Edition
Sue Copley, David Hansell, Jeffrey Kanne
Détails du livre
Aperçu du livre
Table des matières
Citations
À propos de ce livre
The chest radiograph is a ubiquitous, first-line investigation and accurate interpretation is often difficult. Radiographic findings may lead to the use of more sophisticated imaging techniques, such as multidetector computed tomography (MDCT) and positive emission tomography. Containing 100 challenging clinical cases and illustrated with superb, h
Foire aux questions
Comment puis-je résilier mon abonnement ?
Il vous suffit de vous rendre dans la section compte dans paramètres et de cliquer sur « Résilier l’abonnement ». C’est aussi simple que cela ! Une fois que vous aurez résilié votre abonnement, il restera actif pour le reste de la période pour laquelle vous avez payé. Découvrez-en plus ici.
Puis-je / comment puis-je télécharger des livres ?
Pour le moment, tous nos livres en format ePub adaptés aux mobiles peuvent être téléchargés via l’application. La plupart de nos PDF sont également disponibles en téléchargement et les autres seront téléchargeables très prochainement. Découvrez-en plus ici.
Quelle est la différence entre les formules tarifaires ?
Les deux abonnements vous donnent un accès complet à la bibliothèque et à toutes les fonctionnalités de Perlego. Les seules différences sont les tarifs ainsi que la période d’abonnement : avec l’abonnement annuel, vous économiserez environ 30 % par rapport à 12 mois d’abonnement mensuel.
Qu’est-ce que Perlego ?
Nous sommes un service d’abonnement à des ouvrages universitaires en ligne, où vous pouvez accéder à toute une bibliothèque pour un prix inférieur à celui d’un seul livre par mois. Avec plus d’un million de livres sur plus de 1 000 sujets, nous avons ce qu’il vous faut ! Découvrez-en plus ici.
Prenez-vous en charge la synthèse vocale ?
Recherchez le symbole Écouter sur votre prochain livre pour voir si vous pouvez l’écouter. L’outil Écouter lit le texte à haute voix pour vous, en surlignant le passage qui est en cours de lecture. Vous pouvez le mettre sur pause, l’accélérer ou le ralentir. Découvrez-en plus ici.
Est-ce que Thoracic Imaging est un PDF/ePUB en ligne ?
Oui, vous pouvez accéder à Thoracic Imaging par Sue Copley, David Hansell, Jeffrey Kanne en format PDF et/ou ePUB ainsi qu’à d’autres livres populaires dans Medicine et Medical Theory, Practice & Reference. Nous disposons de plus d’un million d’ouvrages à découvrir dans notre catalogue.
Informations
QUESTION 1
1 | A 21-year-old female from Zambia presented with a fever, night sweats and malaise. She had developed the symptoms several weeks before presentation. On examination she was not clubbed and had a slight pyrexia (37.5°C). She was not immunocompromised (CD4 count normal) and had a mild leucocytosis. Her chest radiograph is shown (1). |
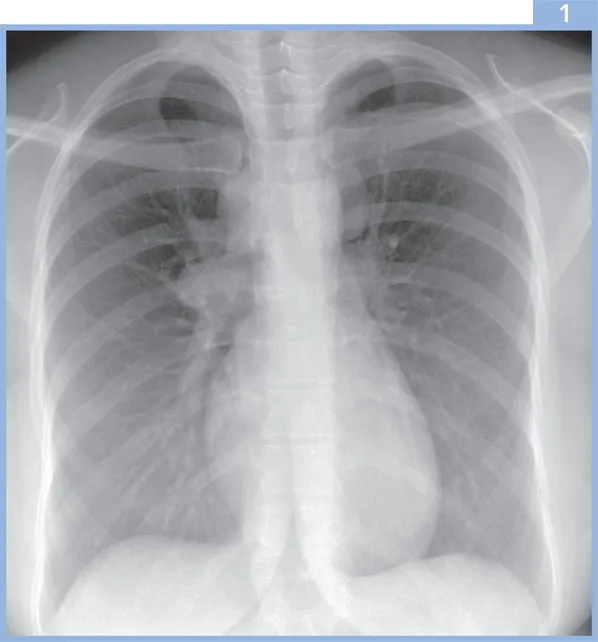
i. | What are the possible diagnoses? |
Answer 1
1i. | The chest radiograph shows right paratracheal, right hilar and left superior mediastinal lymphadenopathy. The diagnosis was primary tuberculosis (TB). The radiological differential also includes lymphoma, metastatic disease (less likely in view of the patient’s age) and sarcoidosis. |
The radiographic features typical of primary TB include a focal pneumonia and lymphadenopathy in the adjacent lymph drainage pathway. The hilar lymphadenopathy is often unilateral with contiguous mediastinal node involvement. Lymphadenopathy may be more prominent in patients of African or Asian origin. The right lung is more commonly involved than the left, and lymph nodes may cause airway narrowing, resulting in segmental or lobar atelectasis. Cavitation has been described in 10–30% of cases. Occasionally, when no cavitation is identified, the radiographic features of primary TB may be indistinguishable from other bacterial pneumonias; however, radiographic abnormalities tend to resolve fairly promptly with appropriate treatment in the latter, whereas radiographic resolution may be slow in TB. The pulmonary disease normally resolves completely, but in approximately 20% of cases, there may be a small calcified residual scar (Ghon focus). The finding may be associated with a calcified mediastinal lymph node (together termed Ranke complex). | |
The radiographic features of pulmonary TB in AIDS depend on the CD4 lymphocyte count. If the count is greater than 200/mm3, the features tend to be those of postprimary TB. However, if the CD4 count is less than 200/mm3, the features are usually those of primary TB, despite the circumstantial evidence that these cases represent reactivation of previously acquired infection. |
QUESTION 2
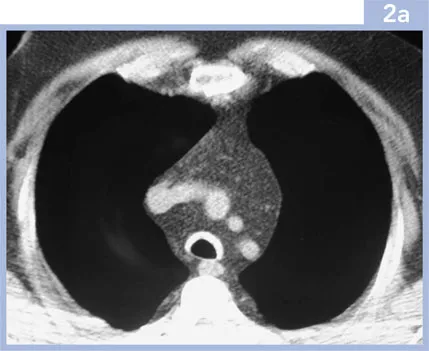
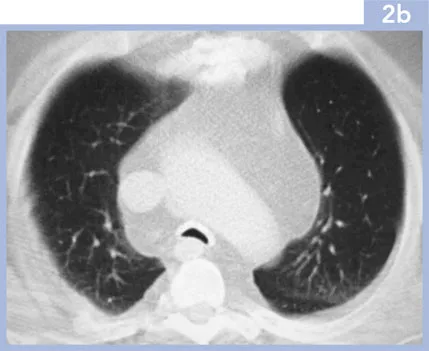
2 | A 60-year-old male presented with dyspnoea, wheeze and stridor occurring several months previously. He had a history of intermittent painful swelling of his auricular cartilage. He had no other relevant past medical history. His blood tests were normal. Lung function tests showed an obstructive defect. The chest radiograph was normal. An inspiratory CT was performed (2a), viewed on soft tissue windows, supplemented with end-expiratory images (2b), viewed on lung windows. |
i. | What is the abnormality? |
ii. | What is the likely diagnosis? |
iii. | What are the treatment options? |
Answer 2
2i. | The CT images show abnormality of the trachea, which is thick-walled and calcified, with sparing of the posterior tracheal membrane. On the end-expiratory images there is tracheal collapse with the posterior membrane bowed anteriorly. Note the excessive mediastinal fat in this patient, who had been treated with corticosteroids for several months. |
ii. | The appearances are those of relapsing polychondritis, a rare disease of unknown aetiology characterised by recurrent inflammation of cartilage. The differential diagnosis includes tracheobronchopathia osteochondroplastica and amyloidosis (which also affects the posterior tracheal membrane, which is spared in this patient). Structures that are most often affected by relapsing polychondritis include the nasal cartilage, the pinna and the cartilage-containing large airways. The disease is commonest in the fifth decade and there is an equal sex incidence. There is an association with other autoimmune diseases such as rheumatoid arthritis. Histopathological findings are chondral and perichondral inflammation with chondrolysis. |
Respiratory tract involvement is a common and potentially life-threatening complication and may involve the large, cartilage-containing airways from the trachea to the segmental bronchi. The stenoses may be multiple, single, dynamic or fixed, and diffuse involvement may occur. The chest radiograph is often normal, although areas of atelectasis may be seen. CT demonstrates airway thickening, calcification and collapse on end-expiration. Multiplanar reconstructions may be useful to guide treatment such as stenting. | |
iii. | The treatment options include long-term steroids (as in this patient) to reduce airway inflammation, although more invasive techniques, such as tracheostomy or airway stenting, may be required. |
QUESTION 3
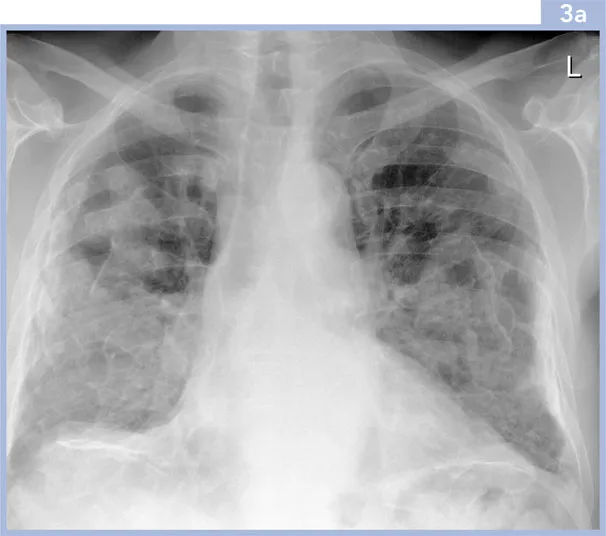
3 | A 67-year-old male presented with a productive cough. He had worked as a packer in an asbestos factory. He had never smoked and did not keep any pets. The patient was well on examination with no abnormal physical signs. Serum biochemistry and full blood count were normal. Spirometric and plethysmographic lung function indices were normal. |
i. | What does the chest radiograph (3a) show? |
ii. | What is the likely cause? |
Answer 3
3i. | The chest radiograph shows irregular confluent opacities projected over both lungs and the diaph... |
Table des matières
- Cover
- Title Page
- Copyright Page
- Table of Contents
- Preface
- List of Abbreviations
- Glossary
- Clinical Cases
- Further Reading & Useful Websites
- Index
Normes de citation pour Thoracic Imaging
APA 6 Citation
Copley, S., Hansell, D., & Kanne, J. (2014). Thoracic Imaging (2nd ed.). CRC Press. Retrieved from https://www.perlego.com/book/1598973/thoracic-imaging-illustrated-clinical-cases-second-edition-pdf (Original work published 2014)
Chicago Citation
Copley, Sue, David Hansell, and Jeffrey Kanne. (2014) 2014. Thoracic Imaging. 2nd ed. CRC Press. https://www.perlego.com/book/1598973/thoracic-imaging-illustrated-clinical-cases-second-edition-pdf.
Harvard Citation
Copley, S., Hansell, D. and Kanne, J. (2014) Thoracic Imaging. 2nd edn. CRC Press. Available at: https://www.perlego.com/book/1598973/thoracic-imaging-illustrated-clinical-cases-second-edition-pdf (Accessed: 14 October 2022).
MLA 7 Citation
Copley, Sue, David Hansell, and Jeffrey Kanne. Thoracic Imaging. 2nd ed. CRC Press, 2014. Web. 14 Oct. 2022.