eBook - ePub
New Therapeutics for Traumatic Brain Injury
Prevention of Secondary Brain Damage and Enhancement of Repair and Regeneration
Kim Heidenreich
This is a test
- 352 pages
- English
- ePUB (adapté aux mobiles)
- Disponible sur iOS et Android
eBook - ePub
New Therapeutics for Traumatic Brain Injury
Prevention of Secondary Brain Damage and Enhancement of Repair and Regeneration
Kim Heidenreich
Détails du livre
Aperçu du livre
Table des matières
Citations
À propos de ce livre
New Therapeutics for Traumatic Brain Injury: Prevention of Secondary Brain Damage and Enhancement of Repair and Regeneration explores traumatic brain injury (TBI), a major cause of death and disability throughout the world. The delayed nature of the secondary injury phase suggests that there is a therapeutic window for pharmacological interventions or other approaches to prevent progressive tissue damage and improve functional outcomes. It is now apparent that therapeutic interventions should entail both protective and repair/regeneration strategies depending on the phase of brain injury.
This book describes emerging experimental strategies for the treatment of TBI, including new anti-inflammatory or anti-apoptotic therapeutics that limit brain damage, and novel or repurposed drugs that enhance repair or regeneration of the brain after injury.
- Comprehensive overview of basic approaches and translational development of new therapies for TBI
- Edited by a prominent TBI researcher that includes contributions by leading global researchers in the field
- Presents a great resource for researchers and practitioners to learn more about the many evolving preclinical studies and clinical trials currently underway, and the challenges of bringing translational studies in TBI to the clinic
Foire aux questions
Comment puis-je résilier mon abonnement ?
Il vous suffit de vous rendre dans la section compte dans paramètres et de cliquer sur « Résilier l’abonnement ». C’est aussi simple que cela ! Une fois que vous aurez résilié votre abonnement, il restera actif pour le reste de la période pour laquelle vous avez payé. Découvrez-en plus ici.
Puis-je / comment puis-je télécharger des livres ?
Pour le moment, tous nos livres en format ePub adaptés aux mobiles peuvent être téléchargés via l’application. La plupart de nos PDF sont également disponibles en téléchargement et les autres seront téléchargeables très prochainement. Découvrez-en plus ici.
Quelle est la différence entre les formules tarifaires ?
Les deux abonnements vous donnent un accès complet à la bibliothèque et à toutes les fonctionnalités de Perlego. Les seules différences sont les tarifs ainsi que la période d’abonnement : avec l’abonnement annuel, vous économiserez environ 30 % par rapport à 12 mois d’abonnement mensuel.
Qu’est-ce que Perlego ?
Nous sommes un service d’abonnement à des ouvrages universitaires en ligne, où vous pouvez accéder à toute une bibliothèque pour un prix inférieur à celui d’un seul livre par mois. Avec plus d’un million de livres sur plus de 1 000 sujets, nous avons ce qu’il vous faut ! Découvrez-en plus ici.
Prenez-vous en charge la synthèse vocale ?
Recherchez le symbole Écouter sur votre prochain livre pour voir si vous pouvez l’écouter. L’outil Écouter lit le texte à haute voix pour vous, en surlignant le passage qui est en cours de lecture. Vous pouvez le mettre sur pause, l’accélérer ou le ralentir. Découvrez-en plus ici.
Est-ce que New Therapeutics for Traumatic Brain Injury est un PDF/ePUB en ligne ?
Oui, vous pouvez accéder à New Therapeutics for Traumatic Brain Injury par Kim Heidenreich en format PDF et/ou ePUB ainsi qu’à d’autres livres populaires dans Psychology et Cognitive Behavioral Therapy (CBT). Nous disposons de plus d’un million d’ouvrages à découvrir dans notre catalogue.
Informations
Sujet
PsychologySous-sujet
Cognitive Behavioral Therapy (CBT)Part I
Interventional Therapies for TBI Previously or Currently in Phase 3 Clinical Trials
Chapter 1
Why Did the Phase III Clinical Trials for Progesterone in TBI Fail? An Analysis of Three Potentially Critical Factors
D.G. Stein1, R.B. Howard2, and I. Sayeed1 1Emory University, Atlanta, GA, United States 2Emory University (Former), Atlanta, GA, United States
Abstract
Despite hundreds of positive preclinical studies and two successful Phase II clinical trials, two large Phase III trials of progesterone treatment for traumatic brain injury were recently ended with no finding of any difference between the test drug and placebo. This chapter discusses some possible reasons for this outcome and proposes returning to Phase II and using a more effective clinical trial design. Specifically, we propose dose and duration of treatment optimization following allometric scaling principles to convert rat mg/kg/day dose to the appropriate human dose. We also propose to verify that the vehicle, at the concentration needed for patients, does not have antiinflammatory or neuroprotective clinical effects. Finally, preclinical animal studies should be conducted to determine whether the lipid vehicles used might alter the drug effects at the required concentrations.
Keywords
Allometric scaling; Progesterone; ProTECT III; SyNAPSe; Traumatic brain injury
Introduction: Progesterone Treatment Showed Promise in Preclinical Research
Although in many animal models of CNS injury, acute-stage treatment with progesterone demonstrated multifactorial benefits in the repair of the damaged brain, the Phase III translation to effective clinical outcome was disappointing. Over 300 preclinical studies listed on PubMed in both male and female subjects demonstrate that, given within the first few days after a traumatic brain injury (TBI), progesterone can modulate the expression of inflammatory cytokines, reduce levels of glutamate toxicity, attenuate both vasogenic and intracellular cerebral edema, prevent apoptosis and necrosis, restore the functions of the blood–brain barrier, and improve functional outcomes on sensory, cognitive, and motor behaviors. At the cellular level, giving progesterone early in the injury cascade can stimulate glial cells to increase myelin formation and restore metabolic function through its effects on the mitochondrial transition pore, and modify calcium channel activity to stabilize cellular metabolism, reducing the cytochemical cascade that can lead to further cell death in the days, weeks, and months after injury.
Progesterone is also known to have growth-promoting properties in the central nervous system. In preclinical experiments, it stimulates the expression and release of neurotrophic factors such as brain-derived neurotrophic factor, nerve growth factor, and insulin-like growth factor, which repair the damaged brain by stimulating neurogenesis, protecting against axonal degeneration, and enhancing synaptogenesis. Many genes involved in the expression of trophic factors and the inhibition of inflammatory cytokines can be regulated by progesterone, because it works through multiple receptor mechanisms throughout the brain. In laboratory experiments, progesterone and its metabolites consistently produce these beneficial effects in the brain and spinal cord after traumatic contusion injuries, nerve crush injuries, diffuse axonal injury, stroke, hemorrhage, cytotoxic injury, and even in degenerative neuropathologies. For a more detailed understanding of how progesterone and its metabolites modulate the cascade of mechanisms leading to both neuronal loss and repair over the course of brain insult, see Arevalo, Santos-Galindo, Acaz-Fonseca, Azcoitia, and Garcia-Segura (2013), De Nicola, Coronel, et al. (2013), Guennoun et al. (2015), Johann and Beyer (2013), Melcangi et al. (2013), Schumacher et al. (2014), and Stein (2013).
Despite a few reports in the preclinical literature showing no benefits of progesterone treatment (Gilmer, Roberts, & Scheff, 2008; Spratt, Tomkins, Pepperall, McLeod, & Calford, 2014; Wong, Gibson, Kendall, & Bath, 2014), with no known toxic effects and so much experimental data supporting its neuroprotective properties, why did this well-known and well-established drug show no translational promise in Phase III clinical trials?
The Phase II Trials
About 10 years ago, two small, single-center clinical trials began to test progesterone in patients with moderate to severe TBI. ProTECT II (Wright et al., 2007) was a randomized, double-blind, placebo-controlled trial that enrolled consenting adult patients of both sexes within 11 h after their injuries with moderate-to-severe Glasgow Coma Scores (GCS) of 4–12 (detail in Table 1.1). A lower GCS score indicates a lower level of consciousness; the best score, 15, represents the best possible outcome.
Patients received standard of practice care plus or minus progesterone treatment by continuous i.v. infusion at 12 mg/kg/day for 3 days in Intralipid vehicle. The frequency of serious adverse events (SAEs) and mortality at 30 days postinjury were the measures of drug safety. The primary measure of functional benefit, also measured only at 30 days post-TBI, was the dichotomized Glasgow Outcome Scale-extended (GOS-E). The Disability Rating Scale (DRS), another quality of life rating-scale measure, was also used. No SAEs were attributable to the progesterone treatment. At 30 days after injury, the progesterone-treated patients with severe TBI (GCS 4–8) remained in coma longer but had a significantly lower mortality compared to patients given only Intralipid. However, upon emerging from their comas, these same patients had somewhat worse GOS-E and DRS scores compared to controls. The investigators speculated that the drug may have increased the incidence of survival in a badly injured treated subpopulation who probably would have died if they had been in the control group. In contrast, the moderately injured (GCS 9–12) TBI patients given progesterone had significantly better 30-day outcomes on the GOS-E and DRS than the placebo group.
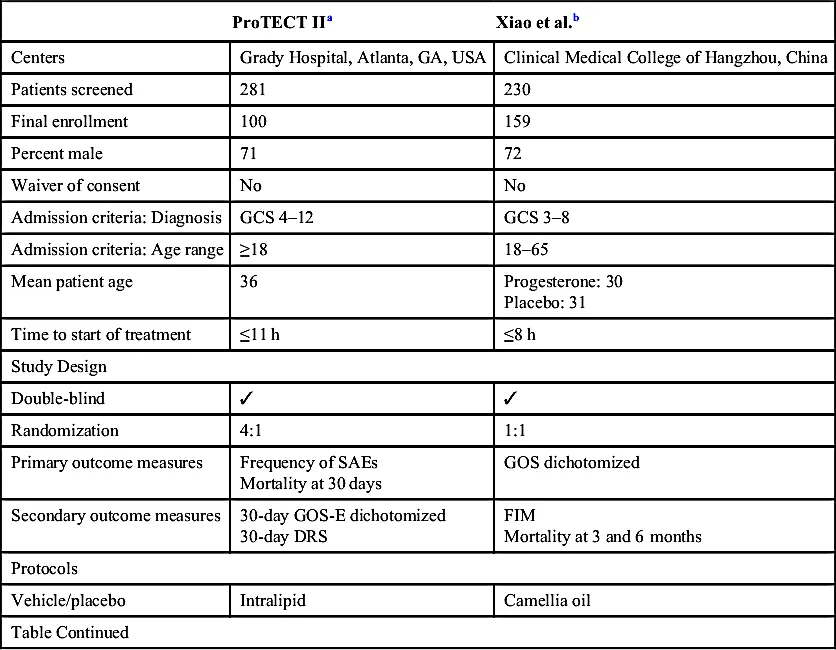
Table 1.1
Phase II Trials
| ProTECT IIa | Xiao et al.b | |
| Centers | Grady Hospital, Atlanta, GA, USA | Clinical Medical College of Hangzhou, China |
| Patients screened | 281 | 230 |
| Final enrollment | 100 | 159 |
| Percent male | 71 | 72 |
| Waiver of consent | No | No |
| Admission criteria: Diagnosis | GCS 4–12 | GCS 3–8 |
| Admission criteria: Age range | ≥18 | 18–65 |
| Mean patient age | 36 | Progesterone: 30 Placebo: 31 |
| Time to start of treatment | ≤11 h | ≤8 h |
| Study Design | ||
| Double-blind | ✓ | ✓ |
| Randomization | 4:1 | 1:1 |
| Primary outcome measures | Frequency of SAEs Mortality at 30 days | GOS dichotomized |
| Secondary outcome measures | 30-day GOS-E dichotomized 30-day DRS | FIM Mortality at 3 and 6 months |
| Protocols | ||
| Vehicle/placebo | Intralipid | Camellia oil |
| Table Continued | ||
| ProTECT IIa | Xiao et al.b | |
| Route of administration | i.v. | i.m. |
| Test drug administration | Total: 3 days at 12 mg/kg/day: Loading dose 0.71 mg/kg/h at 14 mL/h for 1 h, then 10 mL/h of 0.5 mg/kg/h for 11 h, then 5 doses at 10 mL/h to deliver 0.5 mg/kg/h for 11 h | Total: 5 days 1 mg/kg, then once every 12 h for 5 days at 2 mg/kg/day A single-dose volume of 0.05 mL/kg over 5 consecutive days |
| Findings | ||
| Mortality/morbidity | 30 days Severe progesterone 13.2% Severe placebo 40.0% Moderate progesterone 16.7% Moderate placebo 14.3% | 6 months Progesterone 18% Placebo 32% |
| Functional recovery | GOS at 30 days Severe progesterone 21.2% Severe placebo 26.7% Moderate progesterone 55.6% Moderate placebo 0% DRS mean total at 30 days Severe progesterone 10.7 Severe placebo 4.4 Moderate progesterone 5.0 Moderate placebo 12.7 | GOS score at 3 months Progesterone 47% Placebo 31% GOS ... |
Table des matières
- Cover image
- Title page
- Table of Contents
- Copyright
- List of Contributors
- Foreword
- Preface
- Introduction
- Part I. Interventional Therapies for TBI Previously or Currently in Phase 3 Clinical Trials
- Part II. Repurposing FDA Approved Drugs for TBI Treatment
- Part III. Interventional Drugs for TBI in Phase 1–2 Clinical Trials
- Part IV. Interventional Drugs for TBI in Preclinical Development
- Part V. Drugs for TBI Rehabilitation
- Index
Normes de citation pour New Therapeutics for Traumatic Brain Injury
APA 6 Citation
[author missing]. (2016). New Therapeutics for Traumatic Brain Injury ([edition unavailable]). Elsevier Science. Retrieved from https://www.perlego.com/book/1833323/new-therapeutics-for-traumatic-brain-injury-prevention-of-secondary-brain-damage-and-enhancement-of-repair-and-regeneration-pdf (Original work published 2016)
Chicago Citation
[author missing]. (2016) 2016. New Therapeutics for Traumatic Brain Injury. [Edition unavailable]. Elsevier Science. https://www.perlego.com/book/1833323/new-therapeutics-for-traumatic-brain-injury-prevention-of-secondary-brain-damage-and-enhancement-of-repair-and-regeneration-pdf.
Harvard Citation
[author missing] (2016) New Therapeutics for Traumatic Brain Injury. [edition unavailable]. Elsevier Science. Available at: https://www.perlego.com/book/1833323/new-therapeutics-for-traumatic-brain-injury-prevention-of-secondary-brain-damage-and-enhancement-of-repair-and-regeneration-pdf (Accessed: 15 October 2022).
MLA 7 Citation
[author missing]. New Therapeutics for Traumatic Brain Injury. [edition unavailable]. Elsevier Science, 2016. Web. 15 Oct. 2022.