![]()
Biological Base of Frailty
Fielding RA, Sieber C, Vellas B (eds): Frailty: Pathophysiology, Phenotype and Patient Care.
Nestlé Nutr Inst Workshop Ser, vol 83, pp 1-10, (DOI: 10.1159/000382052)
Nestec Ltd., Vevey/S. Karger AG., Basel, © 2015
______________________
Connecting Age-Related Biological Decline to Frailty and Late-Life Vulnerability
Jeremy D. Walston
Division of Geriatric Medicine and Gerontology, Department of Medicine, Older Americans Independence Center, Johns Hopkins University School of Medicine, Baltimore, MD, USA
______________________
Abstract
Frailty is an important construct in aging which allows for the identification of the most vulnerable subset of older adults. At least two conceptual models of frailty have been developed that have in turn facilitated the development of multiple frailty screening tools. This has enabled the study of populations of frail and nonfrail older adults, and facilitated the risk assessment for adverse health outcomes. In addition, using the syndromic approach to frailty, numerous biological hypotheses have been tested, which have identified chronic inflammatory pathway activation, hypothalamic-pituitary-adrenal axis activation, and sympathetic nervous system activity as important in the development of frailty. In addition, age-related molecular changes related to autophagy, mitochondrial decline, apoptosis, senescent cell development, and necroptosis likely contribute to the heterogeneous phenotype of frailty. The recent development of a frail mouse model with chronic inflammatory pathway activation has helped to facilitate further whole organism biological discoveries. The following article attempts to create an understanding of the connections between these age-related biological changes and frailty.
© 2015 Nestec Ltd., Vevey/S. Karger AG, Basel
Introduction
Frailty has long been recognized by health care providers as a syndrome of vulnerability that marks a subset of older adults as being at high risk for adverse health care outcomes, such as functional decline, disability, worsening chronic illnesses, and mortality. Over the past several years, research interest in frailty has grown exponentially as has the interest in integrating frailty into clinical practice models. In addition, marked progress in understanding age-related biological changes has helped to unravel the biology that likely underlies frailty and related biological vulnerability. The purpose of this chapter is to provide a state-of-the-art conceptual overview of frailty and to describe the known physiological and molecular changes that associate with and drive the development of frailty. Further research in this area will help to (1) identify those older adults at highest risk of adverse outcomes, (2) facilitate improved understanding of the biological underpinnings of frailty-related vulnerability, and (3) foster the development of improved preventive and intervention strategies aiming to improve health outcomes and quality of life of older adults.
Frailty Conceptualization
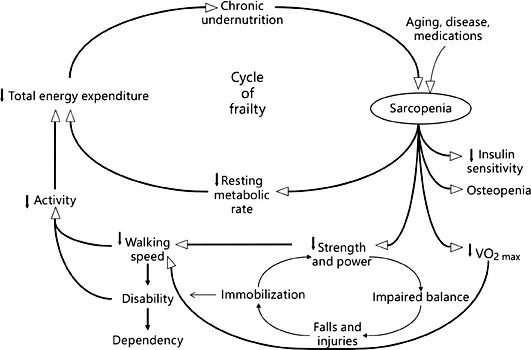
Over the past 20 years, the definitions of frailty have evolved from generalized observations by clinicians that frail individuals were vulnerable, weak, and failing to multiple definitions that have helped to bring scientific rigor to the field of frailty research. At present, two major conceptualizations of frailty have emerged in the literature. The most commonly utilized conceptualization is that frailty is an age-related syndrome with a deep biological basis that becomes manifest during periods of stress [1]. This concept has been further refined into a cycle of decline in energy, skeletal muscles and nutrition that can be triggered by disease, medications, or environmental stressors (fig. 1). This cycle of decline, further influences medical illnesses, mobility, functionality, and cognition. Importantly, this conceptualization has been operationalized into the most commonly utilized frailty screening tool [1] and has allowed for hypothesis testing related to etiology and for intervention development period.
In addition to this biological conceptualization, a cumulative burden conceptualization of frailty has evolved. In this model, frailty is defined by a number of related and unrelated health, biological, social, functional, and cognitive variables that are tallied in an index. Those that are most frail are those with the highest tally of variables [2]. This model has been widely tested for predictive validity and has been shown to capture vulnerability as well as the biological model described above. However, frailty index was not constructed with an underlying biological theory in mind, and hence has not been extensively utilized to test biological hypotheses [2]. Further, because it was not conceptualized around a potential etiology, targeted preventive and intervention strategies have not been developed or tested to date using this model.
Fig. 1. Cycle of frailty that underlies one of the primary conceptualizations of frailty, demonstrating a reinforcing downward physiological spiral that facilitates the development of adverse health outcomes. Reproduced with permission from Walston and Fried [26].
Frailty Measurement
Dozens of studies have been published over the past two decades that detail specific frailty measurement tools [3]. The vast bulk of these tools have been developed to study the risk of adverse outcomes in populations of older adults, and for the most part were developed utilizing aggregate measures of physical function, fatigue, and activity [3]. To date, no clear gold standard for the measurement of frailty has emerged and it is becoming increasingly apparent that none of these tools is adequate for all of the emerging clinical practice, risk assessment, biological research, and intervention development purposes that require frailty screening tools [4]. To date, most of the tools that have been developed can be divided into two groups that match the conceptualization of frailty articulated in the section above, i.e. either tools that attempt to capture essence of a biologically based, syndromic frailty or those that work to capture a tally of deficits or problems that in sum define a level of frailty. A brief summary of commonly utilized measurement tools are discussed below.
Fried et al. [1] previously developed a screening tool that consists of measured grip strength, walking speed, and weight loss along with subjective reporting of activity and fatigue levels. A score of 0-5 is generated based on a series of cutoff points for each measure, with 0 being robust, 1-2 being prefrail, and 3-5 being frail. This tool and adaptations to this tool have been used in population studies of community dwelling older adults to determine demographic information about older adults, and to identify individuals that are at significantly higher risk of adverse health outcomes such as disability, hospitalization, functional decline, and mortality compared to age-matched nonfrail individuals. In addition to this commonly utilized tool, many others have been developed that have a similar construct around syndromic frailty with weight loss, physical function, and skeletal muscle weakness measures most often included in these adaptations. While many have been validated by their ability to predict adverse outcomes in older adults, few have been utilized to test biological hypotheses or interventions.
A second common approach to detecting and measuring frailty comes from Rockwood and Mitnitski [2]. Building on the conceptualization of frailty as a condition that arises from cumulative declines, the tool consists of up to 71 measures of function, illness, cognition, and social mobility. A tally is taken, and those with the highest number of tallies are deemed most frail, and those with the lowest number of tallies are deemed least frail. This tool or similar indexing approaches do not require de novo measurements as information can be abstracted from medical records. Hence, it has been most commonly utilized to assess the risk of an adverse outcome, especially mortality in older adults. Importantly, numerous studies have attempted to include social or cognitive variables into screening tools in order to better capture frailty and its incumbent risk for adverse outcomes in broader population contexts. This will continue to be an important area of development in frailty research [5].
The Biology That Underlies Frailty
In order to better understand the etiology of frailty and late-life vulnerability, and in order to facilitate the development of treatment and prevention strategies, an improved understanding of the connections between age-related biological changes and frailty is required. As mentioned above, the most commonly utilized frailty construct was conceptualized around age-related biological and physiological changes with potential influence from poor nutrition and medical conditions [1]. In older adults, it is apparent that these changes do not exist in isolation; rather they exist together in a variety of constellations, which in sum contribute to frailty and the inherent biological vulnerability observed in frail, older adults [6]. We and others have helped to develop model pathways that have helped to conceptualize the interconnections between age-related biological changes, physiological system changes, and disease states with frailty and adverse outcomes [6]. The following sections detail studies of chronic disease, physiology, and biology that have been performed related to frailty.
Disease States and Frailty
Multiple investigators have attempted to identify important relationships between disease states and frailty in older adults. Early work identified a strong correlation between glucose intolerance and type 2 diabetes mellitus and frailty in older adults [7]. In addition, vascular disease, especially congestive heart failure, has been shown to be highly related to frailty in older adults [8]. Although associations between frailty and disease states do not prove causality, they suggest that a common underlying biological mechanism ties some diseases and frailty together. For example, an important biological commonality that has been identified in frailty and chronic disease is the chronic activation of inflammatory pathways and the strong relationship between inflammation and frailty as detailed below. Other studies have shown heightened activation of clotting pathways and more clotting events in frail older adults, further supporting biological commodity [7, 9]. Many studies demonstrate a substantial overlap between inflammation, frailty, and chronic disease states, including congestive heart failure, hypertension, and diabetes mellitus [7, 8, 10].
Physiological System Dysregulation and Frailty
Dysfunction in multiple physiological systems is thought to play an important role in late-life vulnerability. As biological understanding rapidly evolved, the distinction between physiological and molecular biological sys...