![]()
1
Dermatology and Oncology
![]()
1
Epidemiology and Burden of Disease
Beth N. McLellan1, Devika Patel2 and Mario E. Lacouture3,4
1The Ronald O. Perelman Department of Dermatology, New York University School of Medicine, New York, NY, USA
2Department of Dermatology, Henry Ford Hospital, Detroit, MI, USA
3Dermatology Service, Memorial Sloan-Kettering Cancer Center, New York, NY, USA
4Department of Dermatology, Cornell University, New York, NY, USA
Introduction
Due to recent advances in cancer therapies, patients are now living longer than ever before. For all diagnosed cancers, the 5-year relative survival has increased from 50% in 1975–1977 to 66% in 1996–2004 [1]. From 1990 to 2003, all-site cancer deaths in the United States decreased by 1% per year and these declines were especially pronounced for some of the most common malignancies including breast, prostate, colorectal, and lung cancers [2]. In the United States in 2009, there were 1 479 350 new cancers expected to be diagnosed [1], of which 52–87% were treated with surgery, 24–35% with chemotherapy, and 47–51% with radiation therapy (based on 2002 data for breast, lung, and colorectal cancers) [3]. Fifty to sixty thousand hematopoietic stem cell transplants are performed worldwide per year [4].
The large number of people being diagnosed with cancer in combination with increased survival rates have led to an increased number of patients living with a history of cancer, estimated to be 11.1 million in 2005 in the United States [1], of which 270 000 are survivors of pediatric cancers [5]. The increased number of patients living with and after cancer has revealed a number of dermatologic issues specific to this population: affecting cutaneous health, causing a financial burden, decreasing health-related quality of life, and impairing consistent drug dosing.
Dermatologic health in cancer patients and survivors
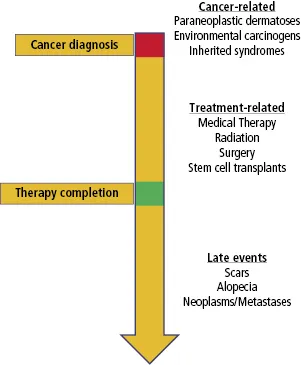
The relationship between the skin, hair, and nails and internal malignancies is manifested in various ways and in all phases of a patient's experience with cancer (Figure 1.1) . Even before a diagnosis of cancer is made, the skin may be affected by genetic syndromes with an increased cancer risk, environmental carcinogens leading to both skin conditions and internal malignancies, or paraneoplastic syndromes. Before treatment begins, patients can be affected by a number of dermatologic problems, most commonly tinea pedis/onychomycosis, pruritus, and xerosis [6]. After the diagnosis of cancer is made, cancer treatments (systemic agents, radiation, therapeutic transplants, and surgeries) can result in a number of skin, hair, and nail adverse events (AEs) that develop either as a result of idiosyncratic reactions or as an effect on rapidly proliferating cells (of which the skin, hair, and nails are prototypical structures).
The number of dermatologic AEs of chemotherapeutic agents is large and continues to expand as new agents come into use (see Appendix 1.1). In 2008, of approximately 384 000 routine AEs for phase I and II studies were reported to the Cancer Therapy Evaluation Program (CTEP) via the Clinical Data Update System (CDUS), 30 834 (8.04%) were dermatologic in nature (personal communication, Clinical Data Update System). Actual numbers of dermatologic AE to therapy may be higher than these estimates because of underreporting and inaccurate grading of AEs [14]. These inaccuracies have at least partly been brought about by difficulty applying existing grading systems to distinct dermatologic AEs, as has been demonstrated with other toxicities [15]. Another difficulty is grading AEs that are of low grade but prolonged duration [16]. Improved reporting of dermatologic AE is expected as focused grading scales are created [17].
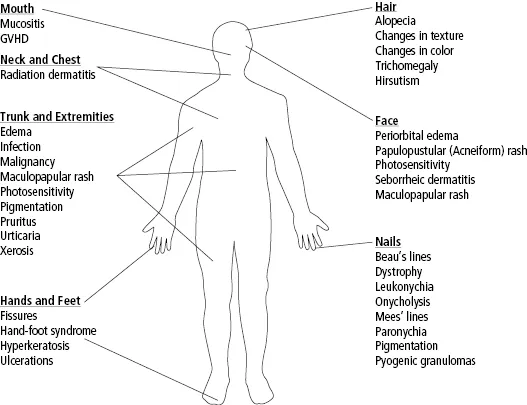
In addition to the primary dermatologic toxicity of therapy, secondary skin infections are a frequent complication. In one study of patients receiving epidermal growth factor receptor inhibitors (EGFRIs), 38% of patients showed evidence of infection at sites of dermatologic toxicities [18]. Treatment modalities other than chemotherapy including radiation therapy, cancer-related surgery, and hematologic transplants are associated with distinct dermatologic toxicities and secondary infections (Figure 1.2).
Financial burden
In addition to the psychosocial effects (discussed in Chapter 6 ), dermatologic AEs also result in a financial cost to patients. Overall costs of treating cancer have increased by 75% from 1995 to 2004 [3]. A portion of this cost can be attributed to supportive dermatologic care. Median medical costs per patient treated for head and neck or nonsmall cell lung cancer with radiochemotherapy are $39 313 per patient with mucositis/pharyngitis and $20 798 per patient without mucositis/pharyngitis [19]. Much of the increased cost was attributed to increased length of hospital stay [19]. For dermatologic AEs in patients treated with EGFRIs or platelet-derived growth factor receptor (PDGFR) and vascular endothelial growth factor receptor (VEGFR) inhibitors, mean cost of treatment for dermatologic toxicities was $2496 per patient [20]. Costs associated with stem cell transplantation can be increased by as much as $28,100 by development of acute graft versus host disease (GVHD) [21]. It is plausible that a prophylactic approach to managing treatment-induced AEs could decrease these associated costs.
Health-related quality of life
All of the described dermatologic toxicities due to cancer treatment can have a significant impact on a patient's health-related quality of life (HRQL). Patients most frequently report dermatologic AE as carrying a negative impact and of being unanticipated prior to therapy, with 67% of patients reporting that dermatologic AEs are worse than their initial belief [22]. Fifty-eight percent of patients rate chemotherapy-induced alopecia as the most traumatic side effect from their therapy and 8% of patients would decline chemotherapy because of fear of hair loss [23]. In a study of breast cancer patients receiving radiation therapy, the skin changes induced by radiotherapy were found to negatively impact physical well-being, body image, emotional well-being, functional well-being, and treatment satisfaction [24]. Scars resulting from oncologic surgical procedures can lead to psychologic problems in 15% of survivors of childhood cancers [25]. In a prospective study measuring the frequency and impact on quality of life of dermatologic toxicities in women receiving chemotherapy, 34% of women reported dermatologic AEs as most important during treatment and they were the most common significant contributor to overall HRQL [26]. Of those who develop dermatologic AEs, 69% feel significantly limited in their daily activities [26].
Dosing of chemotherapy
Perhaps the most imposing challenge offered by dermatologic AE is their ability to result in dose modifications of anticancer therapies. Although the effects of anticancer therapy dose modification on progression-free survival or overall survival have not been evaluated, one can surmise that by reducing dose intensity, clinical outcome will be negatively affected. Studies linking the frequency and severity of dermatologic AEs to a longer median survival underscore the importance of managing dermatologic events, as patients who develop these untoward events are those most likely to benefit from their antineoplastic therapy [27]. Most notably, the papulopustular (acneiform) eruption to the EGFRIs (e.g., erlotinib, cetuximab, and panitumumab) has been shown to correlate with increased progression-free and overall survival in a variety of solid tumors [28,29].
In patients receiving cetuximab for example, up to 11.3% will develop a grade 3 or higher skin rash, necessitating dose reductions [30]. The development of mucositis is shown to lead to a twofold increased risk of chemotherapy dose reduction and limits the ability to give methotrexate for prevention of GVHD following autologous stem cell transplants [31]. Effectively recognizing and treating dermatologic toxicities to chemotherapy can minimize dose reductions and treatment interruptions as shown in the STEPP trial in which 12 doses were delayed in the prophylactic skin treatment arm, compared to 21 doses in the reactive arm [32].
Conclusions
The increasing number of cancer patients and survivors has led to an increased awareness of the HRQL components and treatment-related dermatologic manifestations seen in this patient population. These dermatologic toxicities are diverse and can have an enormous impact on the cutaneous health of patients, overall costs of treatment, healthcare-related quality of life, and consistent anticancer therapy. The recognition of all of these factors has led to a new field within dermatology: supportive oncodermatology, which is focused on the addressing the aforementioned dermatologic issues facing cancer patients and survivors.
References
1 American Cancer Society. (2009) Cancer Facts and Figures 2009. Available from: http://www.cancer.org/downloads/STT/500809web.pdf (accessed 15 April 2010).
2 Byers, T. (2008) Changes in cancer mortality. In: V.T. DeVita, T.S. Lawrence & S.A. Rosenberg (eds), Cancer Principles and Practice of Oncology, 8th ed., pp. 275–282. Lippincott Williams & Wilkins, Philadelphia.
3 Warren, J.L., Yabroff, K.R., Meekins, A. et al. (2008) Evaluation of trends in the cost of initial cancer treatment. Journal of the National Cancer Institute, 100, 888–897.
4 Center for International Blood and Marrow Transplant Research. (2008) 2008 Biennial Report Appendix G – Part 1. Availabl...