![]()
Part 1: Psychology of Reproductive Health
Part I of this book introduces the concept of the psychology of reproductive health. The aim of Chapter 1 is to demonstrate that any biological developments, whether predictable according to normal natural changes or unpredictable or subject to disruption, distortion, disease, discomfort or disability, are influenced by or have an effect on psychological, behavioural, social, cultural and environmental variables. Chapter 2 outlines the conceptual processes and theories of health psychology, providing a suitable background to the reproductive health issues that are discussed in many of the following chapters.
![]()
Chapter 1
Introduction to the Psychology of Reproductive Health
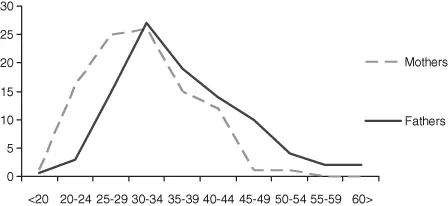
Physiological and genetic factors have long been known to influence reproductive outcome (Galton, 1869). For example, children born to teenage parents or parents of advanced age are at risk of numerous adverse birth and health outcomes (Liu, Zhi and Li, 2011) including well-described disadvantages such as low birth weight and Down syndrome, prevalent in younger and older parents, respectively. However, advanced parental age has also been associated with positive characteristics, such as higher intelligence, in the children. Figure 1.1 (adapted from Ellis, 1926) shows the ages of the parents of 299 ‘eminent’ men to demonstrate that there was a clear majority of elderly fathers among them. More recent research has continued to explore the fascinating early findings of positive effects of parental age on the intellectual abilities of the offspring and alternative explanations have been sought. Influence of parental age on intelligence of the offspring does not seem to be mediated by confounding demographic or other socioeconomic factors (Cohen et al., 1980). Instead, higher maternal age may be more important to superior intelligence test scores in offspring than paternal age (Saha et al., 2009). These inconsistent findings may be due to difficulties defining intelligence, or because testing for intelligence is not sufficiently broad (as it does not include accomplishments, creativity, personality variables and so on). In health or birth outcome terms, the optimum age to have children is 25 to 35 years (Thurstone and Jenkins, 1931), with increasing paternal age resulting in poor outcomes, such as more spontaneous abortions (Kleinhaus et al., 2006) and older maternal age increasing the risks for miscarriage, stillbirth and ectopic pregnancy (Andersen et al., 2000). Both also affect longevity in the offspring (Lansing, 1947), a variable not yet conquered by researchers.
Unlike the early observations of Galton and others in the nineteenth century, research and developments across the twentieth and twenty-first centuries has shown that our survival is increasingly less subject to natural selection. Changes in our behaviours have also brought about changes in our reproductive health. We now use many forms of medicine, both traditional and Western, therapeutic interventions such as organ transplantation and screening in and out of targeted chromosomal characteristics. There are regional, demographic and socioeconomic and behavioural differences in interventions in natural selection, as well as in many other aspects of reproductive functioning.
1.1 Maternal Morbidity and Mortality
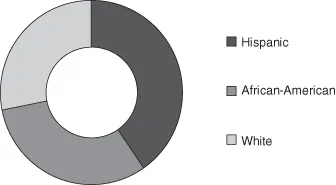
Although women live longer than men (Population Reference Bureau, 2000), they are at a disadvantage because of their reproductive capacity; they can die as a result of pregnancy, labour and delivery, or post partum. It is well known that across the world, maternal mortality and ‘near miss morbidities’ occur disparately between rich and poor countries (Ronsmans and Graham, 2006). Near miss morbidity refers to events that would have resulted in maternal mortality during pregnancy, childbirth or within the 42 post partum days, if medical or other intervention had not occurred (Say, Pattison and Gulmezoglu, 2004). Even within countries, ethnicity confers an increased risk for maternal mortality (CDC, 1999) and for differences between men and women in general (Anderson et al., 1996). Brown et al. (2011) reported significantly higher near miss mortality among Hispanic women than African-American or White women in the USA, see Figure 1.2.
1.2 Age Shifts and Reproductive Consequences
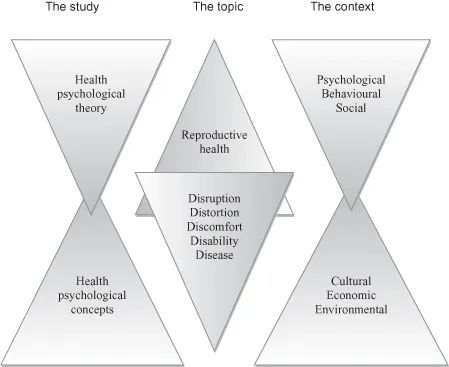
In Europe and the USA, demographic studies have shown age-related shifts in pregnancy timing and numbers since the 1980s (Maheshawari, et al., 2009). Women over the age of 35 are now more likely to present as first-time mothers, and they tend to have fewer children. Accompanying the female age shift in reproduction is a male shift, with women still having children with men of equivalent or older ages. Women’s (and men’s) empowerment, defined as a dynamic process that takes place over time (Lee-Rife, 2010) and that includes resources (e.g. education) and agency (e.g. the ability to act upon goals), affects a person’s interaction with the economic, legal, political, cultural, social and psychological domains. These domains affect health, wellbeing and quality of life. This book will address many of the biological, psychological and behavioural, social and societal, cultural, regional and economic factors impacting upon reproductive health and illness, and their complexities as shown in Figure 1.3.
The complex interactions between individual differences, behavioural, socioeconomic and biological factors are due to numerous components within each of these domains (Table 1.1). Some of these are not easy to pin down, and many are not considered in research and theory investigating aetiological, causal or contributory factors to the development or maintenance of disease or discomfort associated with reproductive events.
Table 1.1 Components within the socioeconomic, individual differences, behavioural and biological domains
| Socioeconomic factors | - Social inequalities
- Cultural and religious differences
- Educational opportunities
- Economic diversity
- Occupational costs and benefits
- Environmental toxicants / pollutants
|
| Behavioural and lifestyle factors | - Smoking
- Drinking alcohol
- Drug use
- Exercising
- Hygiene and health care
|
| Psychological and interpersonal factors | - Personality factors
- Stress
- Vulnerabilities
- Partner, family, friends
- Social support
- Quality of life
|
| Biological / genetic factors | - Racial differences
- Genetics
- Infection
- Disease
- Disability
|
1.3 Interactions between Socioeconomic, Behavioural, Biological and Genetic Factors and Reproductive Health
A number of factors such as the shifts in age at first pregnancy, overall fewer pregnancies and shorter periods of lactation, due to the introduction and use of formula milk, have resulted in a longer lifetime occurrence of menstruation, as described in Chapter 11. Age at menarche declined from 17 to 13 years in Europe between 1850 and 1960 (The Plowden report 1967), with averages across the world differing according to geographic, regional, ethnicity and genetic factors (Tanner and Davies, 1985) – varying from 12.5 in the USA (Anderson, Dallal and Must, 2003) to 16.6 in Iceland (Magnússon, 1978). Timing of menarche is influenced by biological, genetic and environmental factors, including nutrition (see Chapter 5). Similarly, age at menopause (last period) shows variations from 40 to 61 in the Western world, (Minkin et al., 1997) averaging at 51 (Kato et al., 1998), although in the Philippines it is 44 years (Ringa, 2000) (see Chapter 19). The introduction and widespread use of contraceptives, particularly non-barrier contraceptives such as the oral contraceptive pill, has led to an increase in sexual freedom (see Chapter 7), decrease in unplanned pregnancies, altered spacing of children within families, and increased incidences of sexually transmitted and reproductive tract infections. In the developed world, the impact of changes in lifestyle, such as people having sex at an earlier age, delayed conception (Jensen et al., 2004; Waters et al., 2006) and interventions in pre-conception and pregnancy care have all had an effect on reproductive health and fecundability. Although efforts are made to reduce teenage pregnancy, little effort has been spent on the problems associated with delayed or postponed childbearing (Soules, 2003).
1.3.1 Religious Factors
In the developing world, sexual activity and reproduction are less likely to be influenced by liberal Western social conventions about sex and reproduction, but tend to be ruled by religious doctrines and strong cultural influences (as demonstrated in Chapters 7 and 20). Rural Palestinian couples, for example, adhere to Muslim traditions, such as no sex before marriage (Khwaja, 2003), and Muslim couples usually want to start a family immediately after marriage (Rashad et al., 2005). Nevertheless, fecundability within 1 year of marriage is no better than that reported ...