Health care costs make up nearly a fifth of U.S. gross domestic product, but health care is a peculiar thing to buy and sell. Both a scarce resource and a basic need, it involves physical and emotional vulnerability and at the same time it operates as big business. Patients have little choice but to trust those who provide them care, but even those providers confront a great deal of medical uncertainty about the services they offer. Selling Our Souls looks at the contradictions inherent in one particular health care market—hospital care. Based on extensive interviews and observations across the three hospitals of one California city, the book explores the tensions embedded in the market for hospital care, how different hospitals manage these tensions, the historical trajectories driving disparities in contemporary hospital practice, and the perils and possibilities of various models of care.
As Adam Reich shows, the book's three featured hospitals could not be more different in background or contemporary practice. PubliCare was founded in the late nineteenth century as an almshouse in order to address the needs of the destitute. HolyCare was founded by an order of nuns in the mid-twentieth century, offering spiritual comfort to the paying patient. And GroupCare was founded in the late twentieth century to rationalize and economize care for middle-class patients and their employers. Reich explains how these legacies play out today in terms of the hospitals' different responses to similar market pressures, and the varieties of care that result.
Selling Our Souls is an in-depth investigation into how hospital organizations and the people who work in them make sense of and respond to the modern health care market.
eBook - ePub
Selling Our Souls
The Commodification of Hospital Care in the United States
- 248 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
About this book
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
Publisher
Princeton University PressYear
2014Print ISBN
9780691173580
9780691160405
eBook ISBN
9781400850372
{ PART ONE }
PubliCare Rebuffs the Market
As was the case throughout the United States, hospital care in Las Lomas began in the almshouse, tied deeply to the needs of the dependent poor. Hospital care emerged at a time when the categories that would come to distinguish different sorts of dependency from one another—physical and mental illness, illness and old age, disability and poverty—had not been firmly established. And it emerged at a time when the curative capacities of an embryonic medical profession were questionable at best.
The early U.S. hospital can usefully be understood as sitting in opposition to the market, in three related ways. First, institutional care was intended primarily for sick, poor people unable to participate in a burgeoning market economy. The fact that most people of all classes were reluctant to turn to the hospital was in some sense deliberate, a strategy by which community leaders could distinguish the truly needy from those able-bodied poor who could turn to the labor market for their subsistence. As the historian Charles Rosenberg writes, “the hospital’s patients were seen as genuinely needy almost by definition and less likely than recipients of free food or fuel to be impostors, for none but the ill and desperate would willingly seek the dubious comforts of a hospital ward.”1
Second, what little market there was for physicians’ services took place almost entirely outside the hospital. Certainly, hospital appointments became coveted status markers among ambitious members of an emerging medical elite, and a minority of medical students learned their trade by treating the poor in voluntary or municipal hospitals. But paying patients almost always received their care at home; and physicians were almost always prohibited from collecting professional fees in the hospital—even from those patients who paid the hospital for their care.2
Finally, the labor force within the early hospital consisted mostly of recovered patients who, according to Rosenberg, “differed little in background from their charges.”3 Most of these workers were recruited informally, lived within the hospital, and gave the organization an anarchic feel. As a house physician at Massachusetts General Hospital put it in 1857, “There is no system or order & no one knows precisely his duty or keeps to it.”4 Paternalistic impulses and some scientific ambitions were certainly present in the nineteenth-century hospital, but by and large the market was not.
The first hospital in Las Lomas was established in 1859 in the center of town as the second story of the small city jail. According to a local paper, the lower story of the building consisted of “six dark cells, a room for the jailer, and one for petty offenders,” while the upper story was “arranged to accommodate, as comfortably as possible, such indigent persons as may need the assistance of the county, in their sickness.”5 Between 1860 and 1867, the years during which records are available, use of the small hospital grew substantially—from only nine admissions in 1860 to sixty by 1867. All told, between 1860 and 1867, 201 admissions and 37 deaths were recorded. Syphilis, a venereal disease suggestive of moral turpitude, was the most common disease recorded among patients, while the most common cause of death recorded was consumption (or tuberculosis).
The county board of supervisors soon came to regard the facility as inadequate for medical care and, because of its central location, a risk to a public increasingly concerned with contagion. The hospital physician reported, “A more unfavorable location could not well be conceived of, either for the protection of the sick within, or the well without.” The board of supervisors ordered a new stand-alone hospital to be constructed in the northern suburbs of town. This hospital was completed by 1866 and consisted of two stories, with separate wards for male and female patients. While no doubt an improvement from the previous facility, this organization was still a far cry from the hospitals with which we are familiar today. A reporter visiting the new hospital in March 1868 was “highly pleased with the neatness of the surroundings” but nevertheless noted “the necessity of having a dead-house.” As it was, “when of the patients dies his body is placed in the passage-way, where the sick cannot help but see it—anything but a pleasant site—and which does not tend to the improvement of the remaining inmates.”
A report from the hospital physician emphasized moral as opposed to medical concerns.6 Of utmost importance, he wrote, was a “suitable library … for the use of patients … as a most wholesome governmental measure, because even in sickness, idleness breeds dissatisfaction and mischief.” Similarly, a reporter in 1872 highlighted the facility’s social, rather than medical, purposes. After a “careful examination,” during which the reporter spoke with patients “when none of the officers were there,” the only complaint he heard was “in regard to the regulation which requires only two meals a day to be supplied.” The hospital was still, by and large, indistinguishable from a homeless shelter or nursing home; the facility offered medical care, moral training, and basic subsistence simultaneously.
This second facility was similarly short-lived. Both the hospital physician and the board of supervisors had expressed concern about the need to distinguish among different categories of the sick and dependent. There was also worry that this second hospital—which only recently had been on the outskirts of town—had already been enveloped by the expanding city. According to one local history, neighbors had been “passing petitions asking that [the facility] be relocated outside the city limits, citing its odors, the danger of contagion and the loitering of ambulatory patients.”
During the 1870s, then, the county began to shift its care for the poor to a site even farther from downtown: a hundred-acre farm where PubliCare Hospital now stands. It was here where the county consciously undertook the work of distinguishing various categories of dependency. In 1874, the board of supervisors first bought the property to serve as the county farm. The poor would be sent there, while the sick would stay at the hospital. In 1882 it was reported that there were thirty “inmates” at the county farm, while twenty-five still remained at the hospital. A farmer, hired by the county, grew vegetables that could feed the residents of both facilities and be sold as cash crops to help defray the costs. His wife served as the matron of the almshouse, tending to its occupants. As early as 1877 the county had built a “pest house” on the property of the county farm to isolate those with contagious disease, while the board of supervisors began to plan for a new hospital on the same grounds.
Over the course of 1887, a new hospital facility was built on the land. A newspaper article on May 14 of that year gushed with pride about it: “If there is any one thing more than another of which [the] county may justly be proud and to which her citizens may point with pardonable pleasure it is her public institutions … far from being least, her new County Hospital, which is made the subject of this article.” The reporter continued,
As the brow of that long and tedious hill is reached and the low, long roofs of the farm buildings, come into view, the pathetic lines of Will Carleton’s poem, with which all are familiar[,] are brought vividly to mind. It is certainly “Over the Hills to the Poorhouse,” but the scene presents none of the aspects of the bleak and desolate places about which we read in the old New England tales.
The article went on to describe the “gleaming white walls of the new Hospital building,” the “brilliant green of the window-blinds and shadows cast by the ornamental framework of the verandas which afford delicious shade on three sides of the building.” The new hospital boasted a dining room, kitchen, and sitting and reception rooms; multiple wards for both male and female patients; an operating room “located with a view to securing a true and even light”; offices for doctors and a room for the resident steward; and, throughout, “the latest improved ventilating aparatus [sic].” Standing apart from the facility was now a dead house, also to be used as a “dessecting-room [sic].” The reporter concluded that the “building is an ornament to the county, a compliment to the Board of Supervisors and a sanitarium most propitious in its location and purpose.”
Throughout this period, the board of supervisors appointed a single county physician responsible for the patients at the hospital. This physician was paid an annual salary to tend to the indigent, though he continued to see paying patients in their own homes. The steward and matron, meanwhile, lived on the premises and took care of the nonmedical concerns of patients and almshouse residents. The boundaries between almshouse and hospital were porous.7 As late as 1928, reports from the county physician discussed patients who were transferred from the almshouse to hospital or hospital to almshouse. In December 1928, for example, thirteen men from the hospital (out of forty-five discharged) were transferred to the poor farm, while seven men from the poor farm (out of fourteen discharged) were transferred to the hospital. The line between illness and delinquency was also somewhat blurry. In 1894 the county built a two-room building on the property to serve as a “discipline home.” A reporter described its purpose:
Occasionally some old inmate or feeble-minded persons stray off in search of the fountain of eternal youth or walk to the nearest saloon where bitters are dispensed, and some times [sic] get arrested for vagrancy, which costs the county good money. Such stray sheep have to be punished in some way, and it is proposed to confine them in the two-room house with a high fence around it as a salutary lesson.
These facilities may not have been “bleak and desolate places” like the poor-houses of the big cities on the East Coast, but they were still very much a part of movement away from “outdoor relief” or welfare benefits characteristic of the second half of the nineteenth century. As discussed by historians of social welfare and hospital care, early public institutions were erected often with the explicit purpose of deterring the “able-bodied poor” from seeking welfare payments.8 The almshouse and early municipal hospital embodied the “[i]irreconcilable contradictions”9 in the early modern welfare state between the provision of basic rights and the fear of generating dependency. As a historian of Las Lomas put it, the county was “proud of the fact that they took good care of the poor people. At the same time, it’s not exactly something that the Chamber of Commerce is going to advertise. So they’ve always been of two minds.”
The question of moral hazard is one as old as state social welfare programs. If the state provides too much in the way of social entitlements, the perennial argument goes, then people will lose all sense of work ethic or personal responsibility.10 The movement away from “outdoor relief” towards various types of institutional care in the United States was meant to provide for the poor without enabling the pauper.
Staying Public while Going Private
PubliCare had thus been a place of last resort since its founding. In the 1990s, however, the county decided that it could no longer bear the financial burden of care for the uninsured and underinsured. Nevertheless, there was widespread optimism among county officials and local health care executives that, under private management, the right to care could actually be made consistent with the market for care. This optimistic vision was articulated most explicitly in a study of public-to-private hospital transfers spearheaded by the Henry J. Kaiser Foundation—a study that included PubliCare among its cases. The foundation wrote:
To preserve the institution for indigent patients, for whom it was the provider of last resort, those responsible for the public hospitals decided it was necessary to operate the institution for everyone—that is, to use the market to make the hospital financially viable by attracting not only patients who cannot afford to pay, but also those who can.11
In the case of PubliCare, the report concluded, local government did not have the resources to make the capital expenditures necessary to attract paying patients; the hospital was too small an entity to negotiate with organized insurers and physicians’ groups; and the hospital under public governance was at a disadvantage because hospital leaders were “forced to develop and implement long-term competitive strategies in a public forum … and their competitors [could] sit in on their planning meetings.”12 Turning to the market could actually help the county live out its commitment to the poor more fully.
The board of supervisors decided to lease the hospital to Westside Health Corporation, a large statewide not-for-profit health care company. At the time of the hospital’s privatization, many local residents worried that the move would undermine the hospital’s mission of providing care to the poor and make the hospital less publicly accountable. A community coalition led by the area’s largest public-sector union organized a ballot initiative calling for a public vote on the plan. Despite this opposition, however, the county board of supervisors was set in its decision. A county supervisor said of the opposition, “They might think that they are going to win. But if they win, they lose. The hospital just won’t make it much longer.” When the petition had secured enough signatures for a referendum, the board tried (albeit unsuccessfully) to challenge the validity of the ballot measure in court, arguing that the management of the hospital was “too complicated and time-sensitive to turn over to the electorate.” A vote finally occurred almost eight months after the hospital was privatized, at which point voters decided by a three-to-two margin to continue the lease.
Despite public concern, some practitioners at PubliCare felt more hopeful about the privatization—at least when compared with what had preceded it. One ER doctor was particularly critical of the hospital’s prior public governance, attributing its failures to a combination of incompetence and deliberate neglect. First, he suggested, the hospital’s insulation from the market meant that it was fiscally irresponsible—in a socialized system, he asserted, “no one takes responsibility.” He described how at one point it was discovered that millions of dollars’ worth of workers’ compensation reimbursements had not been received because the county had not hired the staff to do the paperwork. This was emblematic of the county’s incompetence. Yet the doctor also believed that the county had deliberately underfunded the public hospital “because the theory in those days was [that] the public [should] not compete against the private sector.” Private medical interests in the county had thwarted public investments: “Anything that we asked for … like social services, or an improvement to the OB wing … was lobbied [against] by the private sector….” While many other doctors, at the time of the transfer, were concerned that Westside Health was “going to kick out all of the homeless and uninsured patients because [Westside was] a big corporation,” this doctor thought that at least Westside Health had “dedicated themselves to doing this.” In his mind, the public mission of the hospital had never been embraced fully by the county: “The county [was] not supporting this hospital; they [didn’t] want this hospital.” The only alternative was for the hospital to try to sustain its mission as a participant in the private market.
When the county decided to privatize the hospital, the board of supervisors had sought to be discerning about buyers. It refused a proposal from a large for-profit corporation—according to the Kaiser Foundation report—because the “hospital’s medical staff was afraid [it] would ‘turn the hospital upside down to make a buck.’ ”13 And it believed it had found in Westside Health a corporation that could pay attention to the bottom line while remaining committed to the hospital’s public mission. In turn, Westside Health was interested in taking over the facility because the company “had a relationship with a physician group in the area, but no local hospital; the lease of PubliCare Hospital was a way to get into the local inpatient market.”14
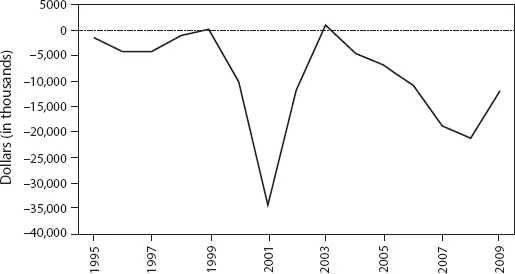
P1.1. ▶ Net income at PubliCare, 1995–2009.
California Office of Statewide Health Planning and Development.
The conditions of the lease were articulated in a health care access agreement, in which Westside Health committed to working “cooperatively and in good faith” to ensure that all residents of the county had access to a “full range of women’s health services (e.g., preventive care, birth control, sterilization, pregnancy termination procedures, labor and delivery) and treatment of HIV/AIDS and other communicable diseases.” Importantly, Westside Health also committed not to “seek additional sums from [the county] to subsidize the cost of Services provided to beneficiaries” of government programs like Medicare and Medicaid.
An underlying assumption, made by both Westside Health and the county, seemed to be that the facility’s financial crisis could be remedied without sacrificing the organization’s public mission. With enough upfront investments and organizational efficiencies, the organization could return to the black. Yet in spite of millions of dollars invested in upgrading the hospital to attract paying patients, PubliCare Hospital had been losing money (excluding capital expenses) under the management of Westside Health in all but two of the fourteen years since the lease had been signed (see figure P1.1).
And while there were several possible explanations for why PubliCare Hospital continued to lose money despite its new investments and new management, the contradiction between the right to care and care as a scarce commodity—a contradiction manifested both in organizational policy and in practitioners’ understandings and practices—is a central part of the story.
{ CHAPTER ONE }
Health Care for All
Sandra Lacks, a social worker at PubliCare Hospital, was an African American woman in her forties, with braided hair tied in a bun behind her head and an authoritative stride. While growing up in a poor section of Boston, Lacks had been introduced to a social worker that “took a liking” to some of her writing and entered her into a citywide speaking contest. Lacks won the contest, and the social worker helped secure a scholarship for her to attend a prestigious East Coast boarding school. “She saw more of me than I saw of myself,” Lacks told me. Making sure Lacks got into boarding school was the social worker’s way of “pulling [her] out of the ghetto.” That social worker’s commitment s...
Table of contents
- Cover Page
- Title Page
- Copyright Page
- Dedication Page
- Contents
- Introduction
- Part One: PubliCare Rebuffs the Market
- Part Two: HolyCare Moralizes the Market
- Part Three: GroupCare Tames the Market
- Conclusion
- Acknowledgments
- A Note on Methods
- Notes
- Bibliography
- Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Selling Our Souls by Adam Dalton Reich in PDF and/or ePUB format, as well as other popular books in Social Sciences & Economic Theory. We have over 1.5 million books available in our catalogue for you to explore.