![]()
1
Examination and Diagnosis
Case 1: Examination and Documentation
Walter S. Krawczyk, DDS, and Anisha K. Thondukolam, DDS
Case 2: Plaque-Induced Gingivitis
Nadeem Karimbux, DMD, MMSc, and Satheesh Elangovan, BDS, DSc, DMSc
Case 3: Non–Plaque-Induced Gingivitis
N. Joseph Laborde III, DDS, and Mark A. Lerman, DMD
Case 4: Gingival Enlargement
T. Howard Howell, DDS, and Maria Dona, DDS, MSD
Case 5: Aggressive Periodontitis
Nadeem Karimbux, DMD, MMSc, Satheesh Elangovan, BDS, DSc, DMSc, and Martin Ming-Jen Fu, BDS, MS
Case 6: Chronic Periodontitis
Case 7: Local Anatomic Factors Contributing to Periodontal Disease
Daniel Kuan-te Ho, DMD, MSc, and David M. Kim, DDS, DMSc
Case 1
Examination and Documentation
CASE STORY
A 40-year-old African-American male (LD) in no apparent distress presented with a chief complaint of: “My dentist told me I have gum disease and I should see a periodontist.” Figures 1–5 are the patient’s intraoral photographs.
LEARNING GOALS AND OBJECTIVES
- The patient’s chief complaint
- Medical and dental history
- Soft tissue and gingival examination
- Periodontal charting
- Radiographic interpretation and diagnosis of periodontal condition
Past Dental History
This patient denied having bleeding gums during brushing or flossing, he had no loose teeth, and he was not in pain. The patient claimed to brush twice a day and flossed sporadically. His last dental visit was a year ago for a cleaning.
This particular patient presented with a blood pressure of 140/90, a pulse of 70 beats per minute, and a respiration rate of 14 breaths per minute. The patient denied having any significant health problems, had no known allergies, and denied taking any medications.
Soft Tissue and Gingival Examination
The patient had no pathologic masses or lesions upon extraoral and intraoral examination (Figures 1–5). He presented with generalized coral pink gingiva with normal pigmentation, scalloped gingival contour with knife-edged margins, pyramidal papillae with localized areas of blunted papilla, stippling, localized areas of recession, and firm consistency with localized edematous areas. There was mild plaque, with no significant supra/subgingival calculus. There was some normal pigmentation associated with the attached gingiva (Figures 1, 4, and 5).
Periodontal Charting
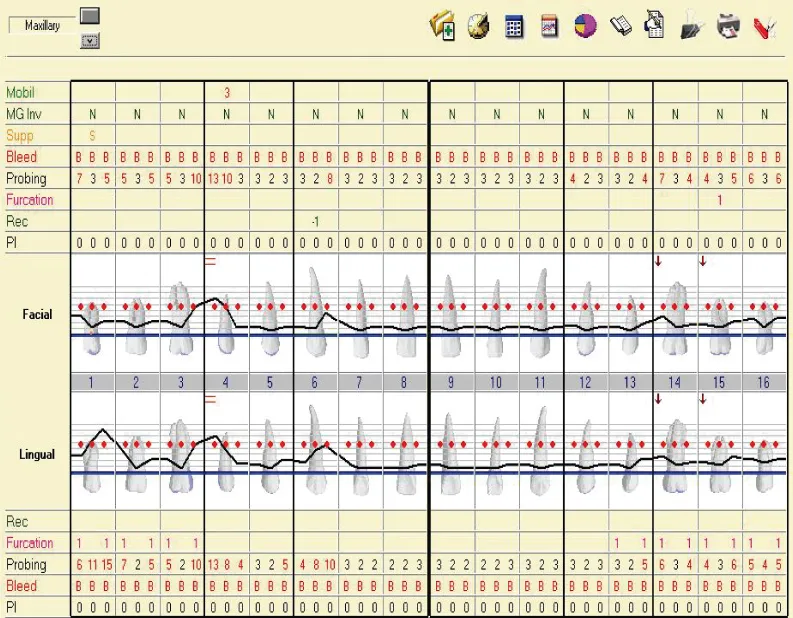
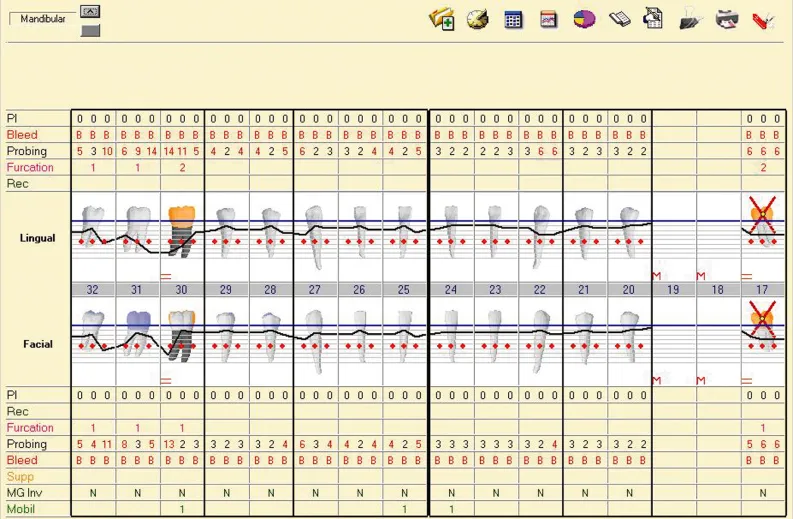
A thorough periodontal examination was completed. The periodontal chart (Figures 6 and 7) shows that the patient had generalized bleeding on probing, minimal plaque, pocket depths ranging from 2 to 15 mm with the more severe probing depths in the posterior teeth, class 1–2 furcations, class 1–3 mobility, and localized recession.
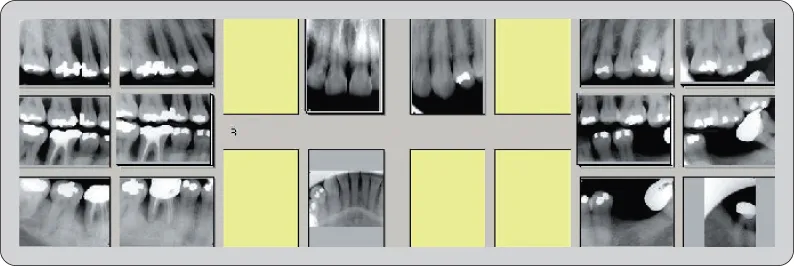
Radiographic Examination
From this full mouth radiograph (Figure 8), generalized bone loss is evident with severe bone loss surrounding #4, #6, #7, and #30. Bone loss in the furcation area is evident for #17 and #30.
Diagnosis
According to the American Academy of Periodontology (AAP), patient LD would be diagnosed with generalized severe chronic periodontitis, which corresponds to an ADA diagnosis of Case Type IV.
Diagnosis (ADA)
Case Type I. Gingivitis
- No attachment loss
- Bleeding may or may not be present
- Pseudopockets may be present
- Only the gingival tissues have been affected by the inflammatory process
- No radiographic evidence of bone loss
- The crestal lamina dura is present
- The alveolar bone level is within 1–2 mm of the CEJ area
Case Type II. Early Periodontitis
- Bleeding on probing may be present in the active phase
- Pocket depths or attachment loss of 3–4 mm
- Localized areas of recession
- Possible class I furcation invasion areas
- Horizontal type of bone loss is most common
- Slight loss of the interdental septum
- Alveolar bone level is 3–4 mm from the CEJ area
Case Type III. Moderate Periodontitis
- Pocket depths or attachment loss of 4–6 mm
- Bleeding on probing
- Grade I and/or grade II furcation invasion areas
- Tooth mobility of class I
- Horizontal or vertical bone loss may be present
- Alveolar bone level is 4–6 mm from the CEJ area
- Radiographic furcations of grade I and/or grade II
- Crown to root ratio is 1 : 1 (loss of a third of supporting alveolar bone)
Case Type IV. Advanced Periodontitis
- Bleeding on probing
- Pocket depths or attachment loss >6 mm
- Grade II, grade III furcation invasion areas
- Mobility of class II or class III
- Horizontal and vertical bone loss
- Alveolar bone level is ≥6 mm from the CEJ area
- Radiographic furcations
- Crown to root ratio is ≥2 : 1 (loss of more than a third of the supporting alveolar bone)
Source: American Academy of Periodontology: Current Procedural Terminology for Periodontics and Insurance Reporting Manual, 7th ed.
Self-Study Questions
A. What dental history questions are important to consider for a periodontal patient?
B. What medical history questions are important to consider for a periodontal patient?
1. From a medical perspective for medical management of the patient
2. From a perspective of conditions that might affect the gingiva/periodontium
C. What constitutes a thorough periodontal examination?
D. How often and what type of radiographs should be exposed for a periodontal examination?
E. How does one come to a diagnosis for gingival and periodontal diseases?
Answers located at the end of the chapter.
References
1. Academy Reports position paper: Tobacco use and the periodontal patient. J Periodontol 1999;70:1419–1427.
2. Haber J, Wattles J, et al. Evidence of cigarette smoking as a major risk factor for Periodontitis. J Periodontol 1993;64:16–23.
3. Emrich LJ, Shlossman M, et al. Periodontal disease in non-insulin dependent diabetes mellitus. J Periodontol 1991;62:123–131.
4. Nelson RG, Shlossman M, et al. Periodontal disease and NIDDM in Pima Indians. Diabetes Care 1990;13:836–840.
5. Academy Reports informational paper: Drug associated gingival enlargement. J Periodontol 2004;75:1424–1431.
6. Rose L, Mealey B. Periodontics: Medicine, Surgery, and Implants. St. Louis, MO: Elsevier Mosby, 2004.
7. Association Report: The use of dental radiographs. Update and...