- English
- ePUB (mobile friendly)
- Available on iOS & Android
Clinical Child Psychiatry
About this book
Clinical Child Psychiatry THIRD EDITION
Making a psychiatric diagnosis in children can be challenging: some clinicians say the incidence of some childhood disorders, such as bipolar disorder and ADHD, is over-diagnosed while others say they are undiagnosed, undertreated, and are a large burden on society. The drug treatment of child psychiatric disorders can also be controversial in children and adolescents. This book fulfills the need for an objective, clinically relevant source to dispel this confusion.
Clinical Child Psychiatry is a textbook of current clinical practice in child and adolescent psychiatry. It is designed as a reference for clinicians that is both easily usable and authoritative, a "chairside" reference for the consultation room.
This book addresses a defined series of clinical entities that represent the bulk of current treatment modalities and disorders encountered in 21st century practice. It is authoritative in the areas addressed while at the same time being rapidly accessible in format. To facilitate access, it presents disorders in declining order of frequency. The authors believe that worthwhile clinical work must be informed by both evidence-based practice and by psychiatry's traditional attention to internal and interpersonal dynamics. They are committed to an approach that is broadly biopsychosocial while based on current clinical evidence for a pragmatic, clinical focus. The book is divided into four sections. The first, Fundamentals of Child and Adolescent Psychiatric Practice, addresses assessment, treatment modalities, and planning. Common Child and Adolescent Psychiatric Disorders and Developmental Disorders cover the diagnosis and treatment of the large majority of disease entities encountered in practice. The final section, Special Problems in Child and Adolescent Psychiatry, includes a variety of topics such as foster care and adoption, loss and grief, and forensics.
- New evidence relating to the areas of depression, psychosis, trauma.
- New insights from genetics, genomics, and proteomics cleverly integrated into chapters on the individual disease with focus on their clinical application.
- New chapter on consultation and collaboration within systems of care.
The book addresses a need for clinicians, many of whom are beginners, non-psychiatrists, or psychiatrists entering unfamiliar territory, to come up to speed rapidly in providing more than perfunctory service to needy populations. This challenge grows ever greater.
Tools to learn more effectively

Saving Books

Keyword Search

Annotating Text

Listen to it instead
Information
| The diagnosis requires evidence of inattention or hyperactivity and impulsivity or both |
| Inattention |
| Six or more of the following symptoms of inattention have persisted for at least six months to a degree that is maladaptive and inconsistent with developmental level: |
| Often fails to give close attention to details and makes careless mistakes |
| Often has difficulty sustaining attention |
| Often does not seem to listen |
| Often does not seem to follow through |
| Often has difficulty organizing tasks |
| Often avoids tasks that require sustained attention |
| Often loses things necessary for activities |
| Often is easily distracted |
| Often is forgetful |
| Hyperactivity and impulsivity |
| Six or more of the following symptoms of hyperactivity and impulsivity have persisted for at least six months to a degree that is maladaptive and inconsistent with developmental level: |
| Often fidgets |
| Often leaves seat |
| Often runs about or climbs excessively |
| Often has difficulty with quiet leisure activities |
| Often is ‘on the go’ or ‘driven by a motor’ |
| Often talks excessively |
| Often blurts out answers |
| Often has difficulty awaiting turn |
| Often interrupts or intrudes |
| Symptoms that cause impairment: |
| Are present before seven years of age |
| Are present in two or more settings (e.g., home, school, or work) |
| Do not occur exclusively during the course of a pervasive developmental disorder, schizophrenia, or another psychotic disorder |
| Are not better accounted for by another mental disorder (e.g., a mood disorder or an anxiety disorder) |
| The criteria are adapted from the Diagnostic and Statistical Manual of Mental Disorders, 4th edition, Text Revision. |
- inappropriate or excessive activity, unrelated to the task at hand, which generally has an intrusive or annoying quality;
- poor sustained attention;
- difficulties in inhibiting impulses in social behavior and cognitive tasks;
- difficulties getting along with others;
- school underachievement;
- poor self-esteem secondary to difficulties getting along with others and school underachievement;
- other behavior disorders, learning disabilities, anxiety disorders, and depression.
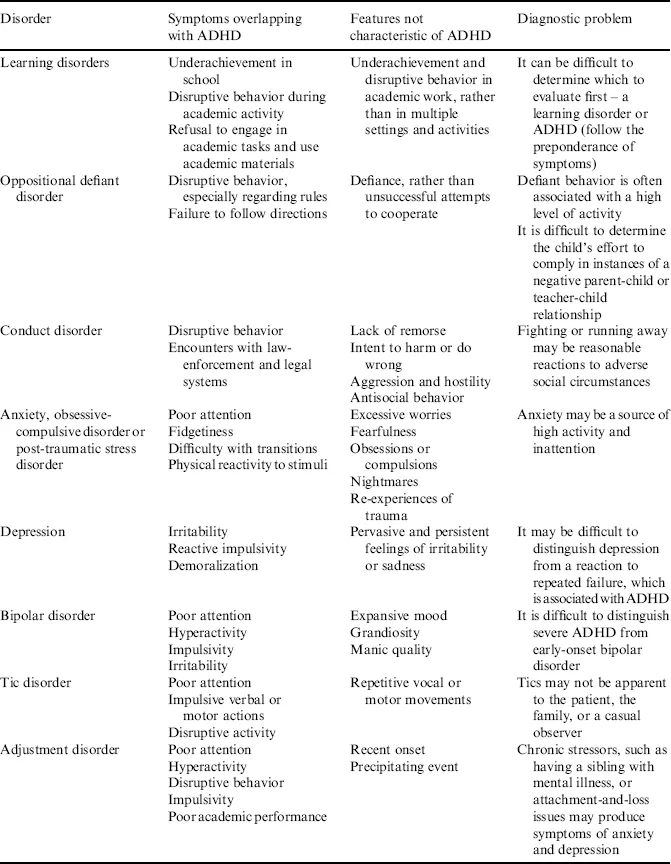
Table of contents
- Cover
- Series Page
- Title Page
- Copyright
- Dedication
- List of Contributors
- Preface to Clinical Child Psychiatry, Third Edition
- Section I: The Fundamentals of Child and Adolescent Psychiatric Practice
- Section II: Common Child and Adolescent Psychiatric Disorders
- Section III: Developmental Disorders
- Section IV: Special Problems in Child and Adolescent Psychiatry
- Index
Frequently asked questions
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.4M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app