![]()
CHAPTER 1
Sketches of the Standard Imaging Modalities
Different Ways of Creating Visible Contrast Among Tissues
“Roentgen has surely gone crazy!”
Different imaging probes interact with different tissues in different ways and yield different kinds of medical information
Twentieth-century (analog) radiography and fluoroscopy: contrast from differential attenuation of X-rays by tissues
X-ray film of a cracked phalange
Generating the beam at the anode of the X-ray tube
Contrast from differential attenuation of the beam within the body
Exposure of a screen-film image receptor
Image intensifier-based fluoroscopy with a CCD/CMOS electronic optical camera
Twenty-first century (digital) images and digital planar imaging: computer-based images and solid-state image receptors
Digital images
Computed tomography: three-dimensional mapping of X-ray attenuation by tissues
Helical, multi-slice CT
Nuclear medicine, including SPECT and PET: contrast from the differential uptake of a radiopharmaceutical by tissues
Radiopharmaceutical = radionucleus + organ-specific agent
Creating contrast through differential uptake of photon-generating radiopharmaceuticals
SPECT and PET
Diagnostic ultrasound: contrast from differences in tissue elasticity or density
B-mode anatomic imaging
Doppler imaging of blood flow
Magnetic resonance imaging: mapping the spatial distribution of spin-relaxation times of hydrogen nuclei in tissue water and lipids
Spin-relaxation times of protons in water and lipids in a strong magnetic field
Mapping the spatial distribution of proton T1 and T2
Appendix: selection of imaging modalities to assist in medical diagnosis
Cardiac versus non-cardiac chest pain
Non-cardiogenic chest pain
Cardiogenic chest pain
Abdominal/pelvis imaging
Abdominal calcifications: non-palpable but seen on radiograph
Head and neck imaging
Musculoskeletal imaging
Vascular imaging
References
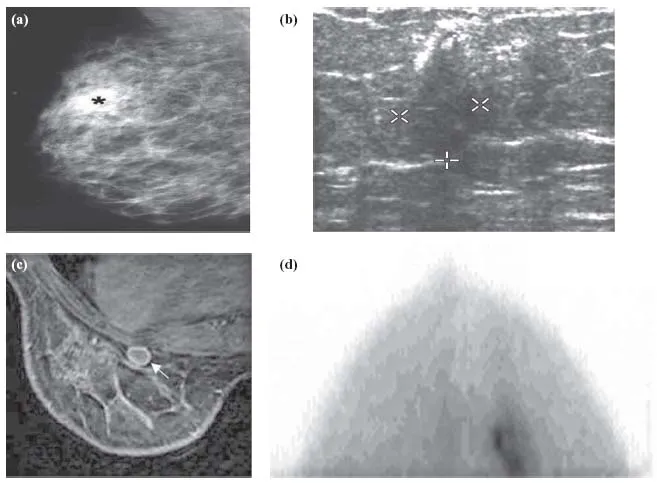
The principal job of a medical imaging modality is to provide clear maps of anatomy, or to make it possible to identify irregularities in physiology, or both (Figure 1.1). It does so by creating contrast among tissues, and the various modalities do this in biophysically diverse ways.
This chapter provides brief sketches of the major imaging technologies that are employed routinely in modern diagnostic clinics to examine the structure and functioning of the body. It begins with modalities slowly developed over the first three quarters of the twentieth century, like screen-film radiography and mammography, image-intensifier tube fluoroscopy, and analog nuclear medicine (NM) and ultrasound (US) imaging. Then came twenty-first century technologies that have flourished only with the advent of high-speed and powerful, but small and affordable, computers – digital planar imaging like computed radiography (CR); digital radiography (DR); digital mammography (DM); digital fluoroscopy (DF), including digital subtraction angiography (DSA); computed tomography (CT), culminating in helical, multi-detector ring CT (MDCT); single photon emission computed tomography (SPECT) and positron emission tomography (PET); advanced forms of B-mode and Doppler US; and magnetic resonance imaging (MRI) in all its glory, with T1-, T2-, and proton density-weighted imaging, functional MRI (fMRI), MR angiography (MRA), diffusion tensor imaging (DTI), and many other variants. All of these modalities will be discussed further in the forthcoming chapters.
“Roentgen has surely gone crazy!”
Although no one realized it at the time, the discovery of X-rays in 1895 foreshadowed the quantum upheavals that would turn the physical sciences upside down in the first quarter of the twentieth century. More immediately and spectacularly, however, it flung open a door that led into a new and completely unanticipated dimension in the practice of medicine − the ability to look non-invasively within a patient's body, without having to cut into it.
A century ago, medical diagnosis was as much art as science. The doctor could measure body temperature, blood pressure, pulse rate, and a few simple chemical attributes of blood and urine, but not much else. Odors and subtle aspects of a patient's appearance during a physical examination often provided equally important clues. But medicine lacked any means to view the interior of the body directly, apart from surgery, to reach critically important diagnoses.
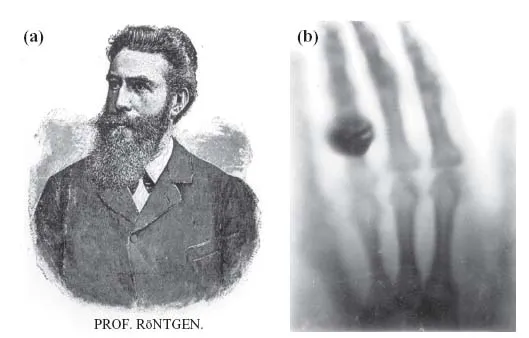
That abiding problem ceased to exist, literally overnight, on the evening of November 8, 1895, when the German physicist Wilhelm Conrad Roentgen chanced upon X-rays (Figure 1.2a). Roentgen, a respectable but little known professor at the University of Würzburg, had been experimenting with an apparatus of widespread scientific interest at the time that is now called a cathode ray tube – a partially evacuated glass tube containing two metal electrodes at its opposite ends that were attached to the outside world by means of a pair of wires passing through the glass. Scientists had been intrigued by what happens when a high voltage is applied between the electrodes: the thin gas within would glow, as would the glass itself in the area near the anode (the electrode attached to the positive pole of the voltage source). It was argued that the agent responsible for this phenomenon was some sort of wave or particle, perhaps negatively charged, that emerged from the cathode (the negative electrode) and that was attracted toward the anode. These so-called “cathode rays” presumably excited the gas and, on striking glass, caused it to fluoresce as well. The nature of cathode rays themselves, now understood to be ordinary electrons, remained obscure for several more years after Roentgen's discovery.
It is not clear what Roentgen was attempting on November 8, since his will stipulated that all of his laboratory notes be burned unread upon his death. In any case, as he worked in a darkened room late in the evening, something unusual caught his eye: when an electric discharge occurred in his tube, a nearby piece of paper that happened to be coated with a chemical compound of barium, platinum, and cyanide produced a glow. With his glass tube completely enveloped in black cardboard, there was no way that visible light from the tube could be reaching the coated paper. So something invisible had to be passing through the cardboard and reaching the barium platinum cyanide, inducing it to give off light. Roentgen had, in fact, discovered X-ray radiation by observing X-ray fluorescence (the emission of light caused by an X-ray stimulus) in a nearby material that was fluorescent. (Patton [1–3] provides a fascinating and detailed accounting of Roentgen's discovery.)
Roentgen was aware that he might have stumbled onto something altogether new, and he was excited and shaken by the remarkable thing he was seeing. But as he explored this totally unexpected phenomenon, he worried that perhaps there might be a simple, obvious explanation that he was overlooking. Far more disturbing was the possibility that perhaps he could not trust his own senses – after all, this appeared to be a physical process that was trivially easy to produce, and undeniably of extraordinary significance, so why had no-one else already seen it and reported it? He knew the physics literature well, and was quite certain that nothing like this had been described before. But were his observations genuine, or might they possibly be the creation of his own mind?
“I believed, ” he later recalled, “that I was the victim of deception when I observed the phenomenon of the ray” [4]. He wrote to his longtime friend, physicist Ludwig Zehnder: “I had spoken to no one about my work. To my wife I merely mentioned that I was working on something about which people would say, when they found out about it, ‘Roentgen has surely gone crazy.’”
But Roentgen persevered. Placing various objects between the tube and the fluorescent screen, he learned that they affected the brightness of the emitted light by different amounts. A few pieces of paper or cardboard had little impact, but a thick sheet of metal quenched the light completely. And when he held his hand in the path of the beam, he could make out the bones of his fingers projected in silhouette upon the screen. A short while later, Roentgen produced the first X-ray record, permanently capturing his wife Bertha's hand and signet ring on a glass photographic plate (Figure 1.2b). Bertha, regrettably, was not overly impressed by the medical significance of the discovery − she had long harbored a terrifying premonition of an early death, and seeing the resemblance of her hand to a skeleton gave her a most unpleasant shock. She ran screaming from her husband's laboratory and never went near it again.
On December 28, Roentgen submitted a paper describing his findings, “On a new kind of ray, ” to a local scientific journal. Within days, news of the discovery was excitedly picked up by the press and spread like wildfire throughout the world, along with the instantly famous picture of Bertha's hand. People found the experiment easy to reproduce, and within months physicians everywhere were using the pictures it produced to set broken bones and to remove bullets and shrapnel. Over the single year following the discovery, more than a thousand technical and medical papers were published on the subject. With his new kind of rays, Roentgen had discovered a splendid window for looking within the living body and painlessly examining organs and bones.
For his work, Roentgen was offered a title, which he refused, and received numerous awards, including the first Nobel Prize in Physics in 1901. Soon af...