Increasingly crowded
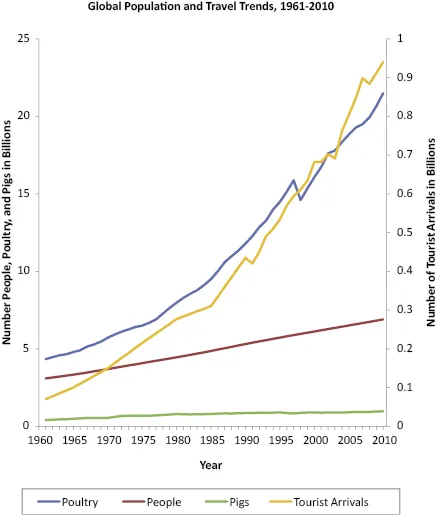
Over the last two centuries, the world's population has increased dramatically. The number of people on earth reached 1 billion sometime around 1804 [8]. After 123 years of growth, the population rose to 2 billion in 1927. Since then, the numbers have increased substantially, reaching 7 billion in 2011 (Figure 1.1). If the population continues to grow at the current rate, there could be around 11 billion people on the planet by 2050. The exponential explosion in numbers has not been uniform across the globe. Importantly, over 80% of the population increase has occurred in less developed countries. Currently, about 60% of the world's population resides in Asia, 15% in Africa, 11% in Europe, 7% in Latin America and the Caribbean, and 5% in Northern America [9]. By 2050, 83% are projected to reside in Asia and Africa.
Much of this growth has occurred in large, dense, population centers. These communities, where the population exceeds 10 million inhabitants, are referred to as “urban agglomerations” or “megacities.” In 1970, there were only two such megacities, but in 2011, there were 23 [10]. Those most recently added to the list of “megacities,” and most likely to accelerate in size, including Lagos, Dhaka, Shenzhen, Karachi, Mexico City, Cairo, and São Paolo, are in developing countries and in tropical and subtropical regions. Residents of these urban agglomerations are, on average, much poorer and younger than in developed settings. Many of these megacities are facing a number of infrastructure and societal challenges, some of which also have implications for the control of influenza in humans and animals. These challenges include healthcare and public health infrastructure limitations, air pollution as a significant contributor to respiratory diseases, concentrations of the poorest of the population living in very crowded conditions, and stressed agricultural supply chains attempting to meet a growing appetite for protein [11,12].
Consider Bangladesh for example. In 2010, there were around 150 million people, a number just under half the population of the United States, living on land the size of the state of Iowa [13]. The population of the capital, Dhaka, was 1.4 million in 1970 [10]. It expanded 11-fold to 15.4 million by 2011. In 2025, this megacity is estimated to increase by another 1.5-fold to around 23 million residents. Dhaka currently is one of the world's most crowded cities. On average, the population density of Dhaka is around 32 600 persons/km2 (84 500/mi2) [14]. In some exceptionally dense areas, such as the slums of Kamalapur, the density rises to 111 325/km2 (288 332/mi2) [15]. Many of the residents in the area are recent immigrants from the countryside, and 44% are under the age of 20 years. In this crowded context with many children, respiratory infections abound. Studies have shown that childhood pneumonia occurs frequently among young children in Dhaka, and influenza and other viral pathogens are identified as the primary cause of these episodes [16,17]. In settings such as these, with the combined contribution of multiple socioeconomic factors and a considerable burden of respiratory illness, seasonal influenza has been identified as an important, and preventable, cause of illness and death.
Dhaka is not alone. Similar megacities are emerging where the promise of employment and a better quality of life continue to draw people to these exceptionally crowded conditions. What does all this mean for influenza among humans? As population density increases, infection transmission potential increases [18]. With a growing number of crowded urban settings, large numbers of younger individuals, and a high frequency of interaction among the population, influenza viruses are given all the right circumstances for efficient and sustained transmission. This is annually evident for seasonal influenza with high attack rates among schoolchildren, college students, military recruits, cruise ship passengers, nursing home residents, and others in densely populated settings. This is also the case with pandemic influenza. Crowded conditions were identified as a significant contributing factor for the 1968 H3N2 pandemic emergence in Hong Kong [19]. Population density and urbanization have been associated with pandemic spread and increased mortality for the 1918 pandemic in the United Kingdom [20]. An increasing population density not only provides an opportunity for influenza to be shared within a community, it also provides opportunities for influenza to be carried to other communities through travelers.
Increasingly connected
The world is more crowded but, just as importantly, it is also more connected. A person can travel to almost any major urban center in the world within the incubation period of influenza [21]. People travel for various reasons, and people are traveling more than ever. For 2011, the projected number of airline passengers was a record-setting 2.75 billion, over 600 million more than in 2006 [22]. Businesses now routinely utilize suppliers and services from distant locations, requiring more global travel. Tourism is also on the rise. From 1950 to 2011, the world's population increased by 2.5-fold, but the number of tourist arrivals increased over 37-fold [8,23] (Figure 1.1). Most increases were in tourists from Asia, and most tourists visited a few highly frequented locations.
The interconnection between communities has an important role in influenza epidemiology. Whereas influenza transmission within communities is predominantly driven by children, transmission between communities is predominantly driven by those who travel frequently, predominately adults. Travelers have been identified as a major contributing factor to the annual cycle of seasonal influenza. In one study, researchers used antigenic and genetic analyses to demonstrate that influenza A (H3N2) virus epidemics for the years 2002–2007 were initiated by influenza viruses originating from East/South-East Asia [24]. The researchers attributed the high frequency of travel and trade from East/South-East Asia to Oceania, North America, and Europe as a likely contributor to the migration of influenza A (H3N2). A lack of travel and trade with South America was suggested to account for the lag in appearance of new viruses to that region.
Tourists have also been identified to contribute to the spread of seasonal influenza. In one report, older travelers from Australia flew to New York City for a cruise to Montreal, likely carrying the influenza A/Sydney/5/97 virus with them [25]. Although this virus had begun to circulate in the Southern Hemisphere, it had not been detected previously in the Northern Hemisphere. The travelers likely infected cruise ship crew members who then infected at least two subsequent cohorts of travelers on the cruise ship. This report demonstrated the potential for travelers to contribute to the global spread of influenza.
Travel has also contributed to the spread of emerging pandemic influenza viruses. Various factors during the 1918 pandemic demonstrate the role of inter-community connections in maintaining the progression of the pandemic. Large-scale movements of military recruits within the United States, and between Europe and the United States, carried the emerging pandemic strain to other naïve populations [26]. Introduction of the virus to crowded military barracks in the United States and in Europe had a devastating impact on the troops. In the Pacific, ship passengers introduced pandemic influenza to remote islanders with substantial impact; Western Samoa suffered the loss of 19–22% of its population [27,28]. Isolated locations in North America were greatly impacted by introduction of the virus [26]. Native Americans had high case fatality rates, reportedly up to 9%. Remote areas of Alaska worked hard to prevent infection from arriving transport ships, but asymptomatic influenza in sailors on departure from Seattle or Vancouver allowed for introduction in port towns throughout the Alaskan peninsula with devastating outcomes. Even infrequent interaction between fur traders and remote Canadian communities was associated with introduction and spread of pandemic H1N1 in 1918 [29].
Almost a century after the 1918 pandemic, the 2009 pandemic H1N1 (A(H1N1)pdm09) influenza virus emerged and its spread was accelerated by international travel. Soon after the detection of the first two recognized cases of A(H1N1)pdm09 in southern California in the United States, additional cases were rapidly reported from Texas, Chicago, Arizona, and New York [30]. In the first reported case series, 18% of patients with A(H1N1)pdm09 in the United States had traveled to Mexico within 7 days of illness onset [31]. Subsequent travel from Mexico, and onward, especially from the United States, led to the spread of A(H1N1)pdm09 to multiple other countries. Researchers have used statistics of airline travel between Mexico and other countries for the 1 March to 30 April 2008 timeframe to see if the locations of the most frequent destinations predicted sites of earliest recognition of A(H1N1)pdm09 in 2009 [32]. During that time period, 2.35 million people traveled from Mexico to over 1000 cities globally. Countries that had received more than 1400 travelers from Mexico were at a significantly elevated risk of importation of A(H1N1)pdm09. Over 80% of travelers from Mexico flew to the United States and Canada. The three most common destinations were Los Angeles (221 494 people), New York City (126 345), and Chicago (111 531).
For many US college students, and families with children in school, travel to Mexico for spring break provided the opportunity for the virus to infect travelers who then returned home and disseminated the novel virus within their communities. One example from early in t...