The book includes basic principles of working in the pathology laboratory including laws and regulations, which must be observed, such as health and safety, data protection and equal opportunities laws and guidelines. Practical exercises are included throughout the book with examples of coursework, suggestions for further exercises and self -assessment. Summary boxes of key facts are clearly set out in each chapter and ideas for group/tutorial discussions are also provided to enhance student understanding.
eBook - ePub
An Introduction to Biomedical Science in Professional and Clinical Practice
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
An Introduction to Biomedical Science in Professional and Clinical Practice
About this book
Biomedical Science in Professional and Clinical Practice is essential reading for all trainee biomedical scientists looking for an introduction to the biomedical science profession whether they are undergraduates following an accredited biomedical sciences BSc, graduate trainees or experienced staff with overseas qualifications. This book guides trainees through the subjects, which they need to understand to meet the standards required by the Health Professions Council for state registration. These include professional topics, laws and guidelines governing clinical pathology, basic laboratory techniques and an overview of each pathology discipline. It helps trainees at any stage of training and in any pathology discipline(s) to think creatively about how to gather evidence of their understanding and professional competence. By referring to specialist sources of information in each area, it helps students to explore particular topics in more depth and to keep up to date with professional and legal changes. It is also of value to any Training Officers who are looking for ideas while planning a programme of training for a trainee biomedical scientist.
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
1
Introduction to a career as a biomedical scientist
1.1 What is a biomedical scientist?
Biomedical scientists are scientifically qualified, registered practitioners who work in clinical pathology departments. They play a vital role in patient care, by carrying out diagnostic tests on samples such as blood, tissue and urine. As healthcare professionals, biomedical scientists work with a range of staff in hospitals and in primary care, to provide clinical laboratory services. About 70% of clinical diagnoses rely on pathology test results. This means that the laboratory work must be performed to the highest possible standards, that the correct specimen type from the right patient must be tested and that the results must be available, to the staff treating the patient, in good time.
Pathology test results are used to:
- Diagnose illnesses. For example, a person with symptoms of tiredness and dizziness might be suffering from iron deficiency anaemia, which could be confirmed by a blood test for haemoglobin concentration.
- Monitor conditions. For example, blood HbA1c levels are regularly monitored in diabetic patients to check that their blood sugar levels are well controlled.
- Screen for diseases in people who are at risk of having the condition, but do not appear to be ill, such as the test for Chlamydia infection.
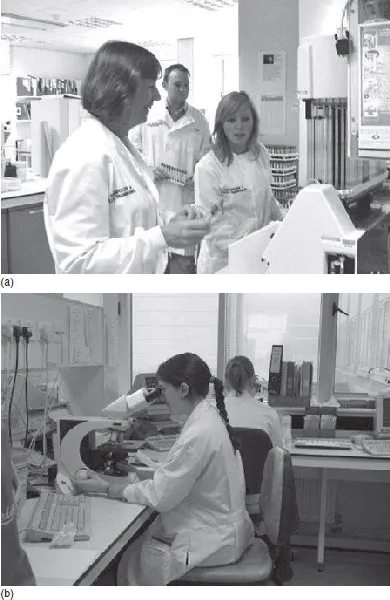
The laboratory testing is performed or supervised by registered biomedical scientists (Figure 1.1), so although they do not have as much direct contact with patients as doctors and nurses, their contribution is vital. If there were not enough nurses available in a particular hospital, individual wards might have to be closed, whereas with insufficient biomedical scientists to run the pathology service, the work of the whole hospital would be compromised. Since the main role of biomedical scientists is to choose the most suitable testing method and then carry out the laboratory work accurately, it is clearly important that they are well trained and work to the highest standards at all times. This means that after the initial training, biomedical scientists have to continue to learn new techniques and keep up to date with scientific advances.
Figure 1.1 (a) Biomedical scientists discuss the operation of a laboratory analyser. (b) Biomedical scientists examine slides prepared from patient samples under a light microscope
A career as a biomedical scientist can be very rewarding, as practitioners use scientific knowledge and technological expertise to help in diagnosis of disease and prevention of illness. They usually specialize in one clinical area of pathology: cytology, clinical chemistry, haematology, histopathology, immunology, medical microbiology, transfusion science or virology, although some posts cover more than one of these areas. In some pathology departments, biomedical scientists are qualified to carry out tests covering several of these areas, such as chemistry and haematology, where the same analyser can be used for all tests (see Chapter 6). Members of staff who are managers, such as quality managers, training managers and overall pathology service managers, need to be familiar with all disciplines, even if they originally trained and qualified in one area. For those who want to progress, there are many possibilities for career development within biomedical science. Some practitioners specialize in a particular technique or disease, through advanced training and scientific research. Others take on roles outside the traditional laboratory setting such as ‘near patient testing’ (see Chapter 2), lecturing at a university or working as a representative for a company which makes laboratory equipment and reagents. Biomedical scientists can also develop expertise as managers, which takes them to senior roles within pathology or the wider health service (see below and Chapter 2).
To qualify as a biomedical scientist, both academic and vocational training are required. The academic part of the qualification in the UK is usually a BSc in Biomedical Science which has been accredited by the Institute of Biomedical Science (see below); the vocational training must be undertaken in a approved training laboratory and is designed to show that the trainee has met the Standards of Proficiency set by the Health Professions Council (see below). It is possible to gain an accredited BSc and then take a post as a trainee Biomedical Scientist to complete the vocational training. However, a number of universities across the UK now offer courses which incorporate the vocational training – the so-called ‘coterminous’ or ‘integrated’ Applied Biomedical Science degree programmes.
1.2 Early development of clinical laboratory sciences
The idea of examining patients’ specimens to aid the diagnosis of clinical disease was used centuries before the underlying science was understood. For example, the ancient literature (from around 1500 BC onwards) includes descriptions of the condition that we now recognize as diabetes mellitus. These relate symptoms of weight loss, extreme thirst and frequent micturation and describe sweet-tasting urine, which implies that someone would test the urine by drinking a little! This seems strange now that we have chemical tests for sugar in the urine (glycosuria) and can observe a colour change rather than a sugary taste, but it is an early example of a how a ‘scientific’ test can confirm a clinical diagnosis when the symptoms are fairly non-specific. Another example is an account from ancient Greek literature by Hippocrates of the progression of the respiratory infection known as ‘consumption’ (i.e. tuberculosis), which describes the patient’s sputum as typically thick, greenish and sweet. A test involving the patient spitting on hot coals was used to determine the prognosis; a characteristic heavy odour noticed in the sputum, when it was heated on the coals, was taken as a sign that the patient would not survive.
From the 16th century onwards, scientific understanding deepened and broadened, as many discoveries were made and laboratory equipment such as microscopes and glassware was refined. This allowed the invention of more specific and reliable clinical diagnostic tests. By the 19th century, with an understanding of chemistry and the knowledge that the ‘sweet taste’ in urine is due to the presence of glucose, it was possible to devise a test for glycosuria. It involved adding a reagent containing copper sulfate to the sample and heating. The sugar acts as a reducing agent, changing the copper sulfate to copper oxide, which causes the solution to change colour from blue to reddish brown. Similarly, by the 1880s, once it had been established that infections were caused by microorganisms, light microscopes were powerful enough to detect them and stains were used to highlight them in samples. In this way, Robert Koch was able to identify a bacterium in the sputum samples of patients with ‘consumption’, which he named Mycobacterium tuberculosis. Both the Benedict’s test for sugars in urine and the Ziehl – Neelson stain for tubercle bacilli are still used in clinical laboratories in many parts of the world today.
By the turn of the 20th century, as the benefits of science to medical diagnosis had become clearer, doctors were increasingly doing tests on patient’s samples. These were usually carried out either by the bedside or in a room nearby that contained the necessary equipment and reagents. The potential for the results of such tests to be used to enhance patient management was recognized and doctors with an interest in laboratory diagnosis started to expand their repertoire. Although there were still some scientists and doctors researching in isolation, there was a demand for diagnostic services from colleagues within hospitals and ‘routine’ testing of samples began in conjunction with research. The work load therefore increased and hospitals began to employ ‘laboratory assistants’, who could collect and examine samples. These laboratory assistants were not medically qualified, but had a high level of scientific and technical training and their work contributed to improvements in accuracy and reliability of testing methods. However, as ‘laboratory assistant’ was not a recognized trade or profession, these workers did not have the protection of a trade union; hospital administrators considered them to be ‘unskilled’ and paid them low wages. Despite this, there are many examples of intelligent and motivated people who made significant, but unheralded, contributions to medical laboratory science at this time. A small selection of the important developments in medical science which affected diagnostic pathology are given in Box 1.1, but there are many other examples.
Box 1.1 Some examples of significant developments in clinical diagnostic pathology
- Development of the Haematoxylin and Eosin stain by Wissowsky in 1876
- Introduction of agar as a bacterial culture medium and use of covered dishes by Koch and Petri in the 1880s
- Invention of the Gram stain by Gram in 1884
- Characterization of the ABO blood group system by Landsteiner in 1902
- Invention of the radioimmunoassay by Yalow and Berson in 1960
- Development of the technique to manufacture monoclonal antibodies by Milstein and Köhler in 1975
- Invention of the Polymerase Chain Reaction by Mullis in 1983
1.3 Development of the biomedical science profession
By the early 20th century, many people were working to provide technical and scientific support for clinical diagnosis in laboratories all over the UK. However, the opportunities for staff working in different laboratories to communicate experiences and ideas were limited and there was a clear need for a professional organization to facilitate this. A laboratory scientist working in Liverpool, Albert Norman, recognized the requirement for such an organization to support his colleagues. Norman consulted with medical colleagues who had formed the Pathological Society of Great Britain and Northern Ireland in 1906, and so had recent experience of founding and running a professional organization. He always believed that the two professional groups should cooperate closely for the good of patient care. Norman founded the Pathological and Bacteriological Laboratory Assistants’ Association (PBLAA) in 1912. The name reflected the nature of the work that laboratory assistants were undertaking at that time. Stains had been developed for use on tissue samples, which allowed the discrimination of cell types and identification of abnormalities when they were examined under the microscope. Agar-based media for the culture of bacteria were also available by this time, which meant that organisms could be grown from patients’ samples and stains were used to help visualize pathogens under the microscope. Some basic biochemical tests were also performed.
In order to be a full member of the PBLAA, a laboratory assistant needed to have undertaken 3 years of training and pay a subscription of 5 shillings (which is 25p in decimal currency but was a considerable amount of money at the time!). Through its members, the PBLAA organized scientific meetings, at which findings from research and developments in diagnostic testing techniques could be shared and also social events. Meeting colleagues under the auspices of the professional body, to discuss scientific issues or just to enjoy each other’s company, is still important for biomedical scientists today. In 1913, the PBLAA started publication of the Laboratory Journal, which was the predecessor of the British Journal of Biomedical Science. Then, as now, the purpose was to provide a journal in which members could publish articles describing their scientific research and improvements in techniques to share with each other. This was even more important in 1913 than it is now, as people did not travel as much as they do in the 21st century for work-related purposes, few people had access to telephones and it would be another 80 years before the Internet was invented!
During the First World War, PBLAA members were often conscripted to the front line rather than to work in field hospitals, because they had no formal professional qualifications. This was obviously a waste of their talents and abilities and so after the War, it was decided to introduce written and practical examinations for laboratory assistants. The first examinations were held in 1921 and covered pathological and bacteriological techniques. The idea was to give structure to training and to ensure that laboratory assistants in all clinical laboratories in the country were operating to the same high standards. In 1937, the professional examination comprised two stages, Part I and Part II. A laboratory assistant who passed Part I was eligible to become an ‘Associate’ of the PBLAA, while the attainment of Part II was necessary to be a ‘Member’ and was a prerequisite for employment in senior posts. A more senior designation of ‘Fellow’ was also introduced. In time, advances in pathological sciences led to people concentrating on haematological investigations, blood transfusion or biochemical tests, to the extent that these became recognized as separate disciplines; examinations in these particular subjects were introduced to reflect this and to support the career development of members working in these areas. During the latter half of the 20th century, further discoveries led to the setting up of more specialized sections within pathology, including immunology, virology and cytology and examinations are now offered in these areas also.
In 1943, the PBLAA changed its name to the Institute of Medical Laboratory Technology (IMLT) and its members were known as ‘medical laboratory technicians’ (MLTs). Professional status for UK members was eventually consolidated by the passing of the Professions Supplementary to Medicine Act in 1960; this made it a legal requirement that MLTs must be registered with the Council for Professions Supplementary to Medicine (CPSM) before practising in the National Health Service. However, by the 1970s, the term ‘technician’ seemed outdated and not a fair reflection of the high levels of training and qualification required to do the job. Members of the profession were involved in research and development in addition to routine diagnostic work and they wanted a title which acknowledged the scientific nature of their work. The IMLT was renamed the Institute of Medical Laboratory Sciences (IMLS) in 1974 and the new professional designation was Medical Laboratory Scientific Officer (MLSO). There were seven grades of MLSO: two training grades, Junior A and Junior B, the Basic grade, Senior, Chief, Senior Chief and Principal. Registration with the CPSM was achieved through an oral examination after a suitable period of training. This was a prerequisite for employment at the Basic grade and Fellowship (see below) of the IMLS was usually needed for someone to be considered for promotion to Senior MLSO. In 1988, the grade system was altered to trainee MLSO, then MLSO 1, 2, 3 and 4.
The IMLS assumed its current name of the Institute of Biomedical Science (IBMS) in 1994, allowing the introduction of ‘Biomedical Scientist’ (BMS) as the professional title. In 2004, the NHS implemented a streamlined structure of pay and conditions called Agenda for Change, which put all staff, apart from doctors and dentists, on the same scales. With this came the current nomenclature of registered practitioner, specialist practitioner, etc., and Bands 5–9 for biomedical scientists in the UK. Over the years, the membership and examination systems have been altered several times in response to the changing needs of the profession. Under the current structure, a person in training could join as an Associate member of the IBMS and progress through Licentiate and then Member, to Fellow during their career. The examination system has been designed to underpin the Agenda for Change grading structure, allowing biomedical scientists to gather evidence of how their professional and scientific knowledge and competency are developing. This is intended to help those who wish to obtain promotion to more senior posts and to take on specialized roles such as quality manager or transfusion practitioner.
1.4 Role of the IBMS as the professional body for biomedical scientists in the 21st Century
The Institute of Biomedical Science (IBMS) is the professional body for biomedical scientists in the UK and its stated aim is ‘to promote and develop biomedical science and its practitioners’ (www.ibms.org). Most current members joined the Institute while training as biomedical scientists in diagnostic laboratories and continued this association as their careers progressed. Thus, while the membership mainly comprises practitioners in clinical laboratories, staff in specialized diagnostic laboratories, researchers and lecturers are also IBMS members. Academic staff, sales representatives and others who are interested in the work of the Institute are also able to join. The main roles of the IBMS are summarized in Box 1.2.
Box 1.2 Roles of the Institute of Biomedical Science (IBMS)
The main roles of the IBMS are to:
- Set professional standards of conduct and practice for members
- Prom...
Table of contents
- Cover
- Contents
- Title Page
- Copyright Page
- Dedication
- Preface
- Acknowledgements
- 1 Introduction to a career as a biomedical scientist
- 2 Organization of pathology departments and the role of pathology in healthcare
- 3 Communication for biomedical scientists
- 4 Quality management in the clinical laboratory
- 5 Basic principles of working in a clinical pathology laboratory
- 6 Introduction to the biomedical science disciplines
- 7 Biomedical science laboratory techniques
- 8 Development of knowledge and competency for biomedical scientists
- Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access An Introduction to Biomedical Science in Professional and Clinical Practice by Sarah Jane Pitt,Jim Cunningham,Sarah J. Pitt in PDF and/or ePUB format, as well as other popular books in Biological Sciences & Human Anatomy & Physiology. We have over 1.5 million books available in our catalogue for you to explore.