This is the first textbook of its kind to offer students an introduction to best practices for using technology in health promotion programs. Integrating detailed case studies and interactive skill-building exercises throughout, this succinct and practical text teaches students to identify the most appropriate technology to meet their goals.
Chapter 1: A Primer on Technology-Based Health Promotion
Chapter 2: Ethical Issues in Technology-Based Health Promotion
1
A Primer on Technology-Based Health Promotion
CHAPTER OVERVIEW
This chapter introduces readers to the use of computers, the Internet, mobile phones, and mobile devices in health promotion. We offer specific examples from a growing body of literature that illustrate how these modalities are unique and different from traditional health promotion efforts. We also offer examples from the literature that illustrate the challenges we face with technology-based health promotion. This dynamic field has offered us several programs that we can highlight as current “best practices,” and we will describe these as well. In this section, we will also consider the role of theory in technology-based health promotion, offering a conceptual framework to link the unique aspects of this field to health promotion generally. Finally, we consider emerging trends in technology-based health promotion. After reading this chapter, the reader should be able to (a) summarize unique elements of technology-based health promotion; (b) identify current “best practices” in computer, Internet, mobile phone, and mobile devices to promote health; (c) describe limitations to technology-based health promotion; (d) identify theoretical concepts that should be considered in development and implementation of technology-based health promotion efforts; and (e) describe emerging trends in the field.
WHAT IS UNIQUE AND BENEFICIAL ABOUT TECHNOLOGY-BASED HEALTH PROMOTION?
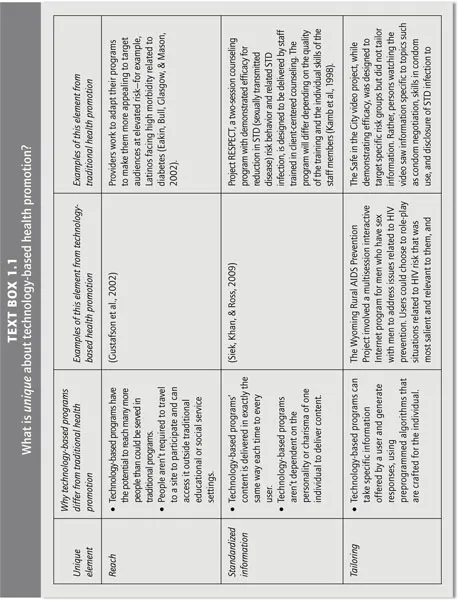
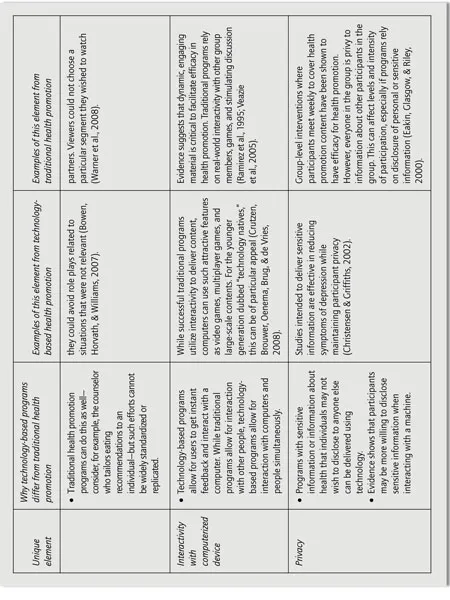
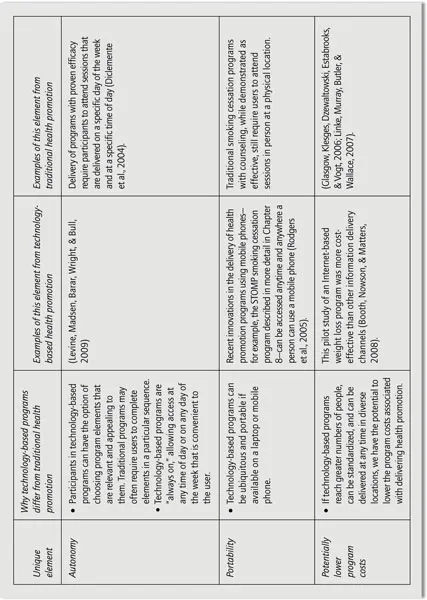
Efforts to promote health are obviously not new. We emphasize that our role in this textbook is not to describe health promotion generally but rather to consider what is unique and different that technology can add to our efforts to promote health. In this segment we consider these unique features of technology-based health promotion by reviewing selected publications that exemplify this point. Text Box 1.1 identifies the key unique elements of technology-based health promotion we describe in this chapter, and the Appendix (p. 236) offers a brief review of selected technology-based health promotion programs that exemplify the points we make in this chapter.
Reaching Larger Numbers With Health Promotion Programs—Including Disadvantaged and Marginalized Groups
One of the most significant contributions technology-based health promotion programs offer is reach. The Internet offers unprecedented opportunities to reach large numbers of people with health promotion programs. With the advent of the Internet (aka the World Wide Web) and browsers designed to search webpages, health promotion entered a new era. The Pew Internet & American Life Project reported that in 2000, there were 52 million Americans who had gone online seeking health information; that number had risen by 2002 to 73 million and by 2006 to 113 million (Fox & Rainie, 2000; Horrigan, 2004; Pew Internet & American Life Project, 2006).
Whereas computers could be used effectively by health care providers to promote health in clinic settings, individuals could now be proactive in seeking health information, and could do so in the privacy of their own homes, on their own time. Programs can now be delivered to people outside traditional clinic, educational, and social service settings, and therefore, they may have the potential to reach people who do not have access to any of these settings.
There remains evidence of a digital divide; that is, poor persons and persons living in resource-poor settings do not have equal access to the equipment used for technology-based health promotion or the levels of bandwidth required to deliver high-quality and graphic-rich content. This suggests that technology-based programs may actually be problematic in that they could bias the delivery of programs to those with computer access and high-speed Internet access. We further discuss this particular limitation of technology-based health promotion in the section on “bias and the ongoing digital divide” below. Of note, however, is recent evidence of a reverse digital divide—wherein lower-income populations and those residing in resource-poor settings are among the fastest-growing consumers of mobile phones, airtime minutes, and text messaging (Cellular-News, 2006). When we consider reach with technology-based health promotion, it is certainly valuable to consider the possibility of even greater penetration and reach into potentially higher-risk groups using mobile phones. Chapter 8 focuses specifically on case studies of health promotion using mobile phones.
Why is reach in health promotion of such critical importance? Consider the classic argument of public health impact. Our health promotion programs are often evaluated to determine if they work—or whether they have efficacy. Public health researchers are also concerned about other factors, including whether they can work for a large and diverse number of people—that is, whether they are effective. Ultimately, if programs have a high degree of efficacy but they work for only a small number and/or select group of people, they will have less impact. Programs that may have relatively lower efficacy but whose effects can be realized by larger and more diverse groups of people will have greater impact overall. This impact is of critical importance, because without it, we cannot hope to affect reductions in morbidity and mortality and improve health.
References
Booth, A. 0., Nowson, C. A., & Matters, H. (2008). Evaluation of an interactive, Internet-based weight loss program: A pilot study. Health Education Research, 23, 371–381.
Bowen, A., Horvath, K., & Williams, M. (2007). A randomized controlled trial of Internet-delivered HIV prevention targeting rural MSM. Health Education Research, 22, 120–127.
Christensen, H., & Griffiths, K. M. (2002). The prevention of depression using the Internet. Medical Journal of Australia, 777(Suppl.), 122–125.
Crutzen, R., de Nooijer, j., Brouwer, W., Oenema, A., Brug, j., & de Vries, N. K. (2008). Internet-delivered interventions aimed at adolescents: A Delphi study on dissemination and exposure. Health Education Research, 23, 427–439.
Diclemente, R. j., Wingood, G. M., Harrington, K. F., Lang, D. L., Davies, S. L., Hook, E. W., lll, et al. (2004). Efficacy of an HIV prevention intervention for African American adolescent girls: A randomized controlled trial. JAMA, 292, 171–179.
Eakin, E. G., Bull, S. S., Glasgow, R. E., & Mason, M. (2002). Reaching those most in need: A review of diabetes self-management interventions in disadvantaged populations. Diabetes/Metab Research and Reviews, 18, 26–35.
Eakin, E. G., Glasgow, R. E., & Riley, K. M. (2000). Review of primary carebased physical activity intervention studies: Effectiveness and implications for practice and future research. Journal of Family Practice, 49, 158–168.
Glasgow, R. E., Klesges, L M., Dzewaltowski, D. A., Estabrooks, P. A., & Vogt, T. M. (2006). Evaluating the impact of health promotion programs: Using the RE-AIM framework to form summary measures for decision making involving complex issues. Health Education Research, 21, 688–694.
Gustafson, D. H., Hawkins, R. P., Boberg, E. W., McTavish, F, Owens, B., Wise, M., et al. (2002). CHESS: 10 years of research and development in consumer health informatics for broad populations, including the underserved. International Journal of Medical Informatics, 65, 169–177
Kamb, M. L, Fishbein, M., Douglas, J. M., Jr., Rhodes, F., Rogers, J., Bolan, G., et al. (1998). Efficacy of risk-reduction counseling to 0prevent human immunodeficiency virus and sexually transmitted diseases: A randomized controlled trial. Project RESPECT Study Group. JAMA, 280, 1161–1167
Levine, D., Madsen, A., Barar, R., Wright, E., & Bull, S. (2009). Asynchronous focus groups on MySpace: Creating cultural and environmental relevance for hard-to-reach populations. Unpublished manuscript.
Linke, S., Murray, E., Butler, C., & Wallace, P. (2007). Internet-based interactive health intervention for the promotion of sensible drinking: Patterns of use and potential impact on members of the general public. Journal of Medical Internet Research, 9, e1O.
Ramirez, A. G., McAlister, A., Gallion, K. J., Ramirez, V., Garza, I. R., Stamm, K., et al. (1995). Community level cancer control in a Texas barrio: Part I. Theoretical basis, implementation, and process evaluation. Journal of the National Cancer Institute Monographs, 117–122.
Rodgers, A., Corbett, T., Bramley, D., Riddell, T., Wills, M., Lin, R. B., et al. (2005). Do u smoke after txt? Results of a randomised trial of smoking cessation using mobile phone text messaging. Tobacco Control, 14, 255–261.
Siek, K., Khan, D., & Ross, S. (2009). A usability inspection of medication management in three personal health applications. Proceedings of Human Computer Interaction International, 1, 129–138.
Veazie, M. A., Galloway, J. M., Matson-Koffman, D., Labarthe, D. R., Brownstein, J. N., Emr, M., et al. (2005). Taking the initiative: Implementing the American Heart Association Guide for Improving Cardiovascular Health at the Community Level: Healthy People 2010 Heart Disease and Stroke Partnership Community Guideline Implementation and Best Practices Workgroup. Circulation, 112, 2538–2554.
Warner, L., Klausner, J. D., Reitemeijer, C., Malotte, C. K., O’Donnell, L., Margolis, A. D., et al. (2008). Effect of a brief video intervention on incident infection among patients attending sexually transmitted disease clinics. PLoSMed, 5, 919–927.
Several researchers have paid close attention to public health impact. Thyrian and Ulrich (2007) argue that a program that can produce an effect on a specific behavioral outcome such as smoking will not necessarily have a substantial impact on smoking prevalence in the population or subsequently on smoking-related morbidity unless it can be designed to reach many people and unless those people can remain engaged with the program over time. Other researchers emphasize the same—unless we can reach large proportions of the audience targeted for a health promotion endeavor, they argue, our program will have limited impact regardless of efficacy (Glasgow, Klesges, Dzewaltowski, Estabrooks, & Vogt, 2006; Klesges, Estabrooks, Dzewaltowski, Bull, & Glasgow, 2007). Glasgow and colleagues take this argument further— they also consider that reach to individuals is indeed critical for program impact, but in addition, they consider that in order to achieve improvements in reach we need to make programs easy for organizations and communities to adopt and to implement. It isn’t enough to reach large proportions of a target audience; in order to sustain program effects over time, you must ensure that organizations coming in contact with a target audience can easily adopt and implement a program (Glasgow, Lichtenstein, & Marcus, 2003).
How exactly would this be relevant for a technology-based health promotion program? Using technology in health promotion certainly has potential for reaching many more individuals than may otherwise participate in traditional face-to-face programs in clinics, schools, and community settings. Using technology could also be appealing for organizations in that technology-based programs (such as a CD-ROM or Internet program) may require fewer human resources to implement than other programs (e.g., a six-session group counseling program for weight loss may require personnel time and clinic space; a similar CD-ROM program only would require a computer and perhaps a short amount of staff time to introduce and orient a patient or participant to the program).
Thus, while it is of course important that our programs show positive effects, it is only by disseminating these effects widely that we will achieve our goals of health promotion and disease prevention. The importance of program reach cannot be overstated (Glasgow, McKay, Piette, & Reynolds, 2001). Consider the following references for a more detailed exploration of public health impact (Dzewaltowski et al., 2010; Klesges et al., 2007; Thyrian & Ulrich, 2007); included in these resources are specific calculations for quantifying the impact of a program.
Standardizing Information
Another advantage offered by technology-based health promotion is that of standardization in program delivery. By offering health promotion via computers, early innovators in this area were able to demonstrate fidelity and standardization as key advantages in the use of technology. Because program content is delivered in the exact same way each time, it removes reliance on individuals for health promotion whose skills and demeanor may be unique and difficult to duplicate (Prochaska, DiClemente, Velicer, & Rossi, 1993; Strecher et al., 1994; Taylor, Houston-Miller, Killen, & DeBusk, 1990).
Tailoring Information
In addition to standardization, another important element of technology-based programs is tailoring. The emergence of computer software and “expert systems” allows for the production and dissemination of individually tailored print material (Bental, Cawsey, & Jones, 1999; Campbell, Peterkin, Abbott, & Rogers, 1997; Campbell et al., 1994; de Vries & Brug, 1999; Kreuter & Strecher, 1996; Lipkus, Lyna, & Rimer, 1999; Marcus et al., 1998; Rakowski et al., 1998; Rimer et al., 1999; Rimer & Glassman, 1998; Skinner, Siegfried, Kegler, & Strecher, 1993; Skinner, Strecher, & H...
Table of contents
Cover Page
Dedication
Title Page
Copyright
Brief contents
Detailed contents
Preface
About the Authors
Part I:Orientation To Technology-Based Health Promotion
Part II: Unique Aspectsof Technology-Based Program Development, Implementation, And Evaluation
Appendix: Technology-Based Health Promotions
Author Index
Subject Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.4M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
Both plans are available with monthly, semester, or annual billing cycles.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go. Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Technology-Based Health Promotion by Sheana Bull in PDF and/or ePUB format, as well as other popular books in Medicine & Nursing. We have over one million books available in our catalogue for you to explore.