![]()
SECTION I
PRINCIPLES
![]()
CHAPTER 1
INTRODUCTION
Patients in the ICU are the most critically ill patients in the hospital. They are usually supported by many different types of mechanical devices and generally have many monitoring lines, tubes, and catheters. Critical management of these patients can change from minute to minute. Physicians depend on the physical examination of their patients, which is often quite difficult, and the portable chest radiograph to help understand the patient’s problems. While CT and ultrasound can be of enormous help with these sick patients, the portable chest radiograph is the most helpful and most commonly used x-ray examination. The malposition of lines, tubes, and catheters and cardiopulmonary complications, such as atelectasis, pneumonia, failure, and effusions, are often initially detected on the portable film.
One of the more frightening experiences for a 1st-year resident is to be summoned to the ICU in the middle of the night as the result of a marked deterioration of a patient. A portable chest x-ray is generally obtained, which reveals a plethora of tubes, lines, and mechanical-assist devices as well as a multitude of cardiopulmonary problems manifested in many different guises. Compounding the problem is the fact that a portable film often does not have the technical quality of films obtained in the radiology department, and there is no radiologist available to help the resident make important lifedeciding decisions.
Very little attention has been paid to teaching medical students, residents, and ICU nurses how to approach and read an ICU film. The purpose of this book is to address the more common problems a student will encounter. Attention to the issues and clinical problems that are displayed herein should provide the student with the framework for intelligent and, I hope, accurate interpretation of the changes seen on chest film found in these patients. This book should help the student identify and correct any abnormal positions in the various devices inserted into the vascular and respiratory systems and identify abnormalities of the cardiopulmonary system.
The book consists of a series of chapters discussing various issues, including how to obtain a proper film and the more common clinical problems encountered each day in an ICU. The accompanying CD has one to nine cases relating to the topics covered in each chapter. Cases are presented that simulate common problems in the ICU. Each case has a short clinical history followed by a portable radiograph. Each case is the result of a sudden change in a patient’s condition, which resulted in an x-ray being obtained. The reader is encouraged to look at the radiograph, identify the various problems, determine the clinical condition that caused the deterioration in the patient, and plan what to do about the problems discussed. I have been teaching this course as part of the 4th-year radiology elective at the University of Connecticut Health Center for 5 years. As I explain the situation to the students, it is 2:00 a.m. and the nurse in the ICU has just awakened you to tell you that one of your patients has crashed. The reader tells the nurse to get a chest radiograph and arrives 5 minutes later in the ICU. What do you see and what are you planning to do about it? That is the name of the game.
After studying at the radiograph, the student should turn to the discussion of the findings, which includes an interpretation of the problems found and an outline of the course of action to be followed. It is hoped that this will help the reader solidify the concepts presented in Section I of the book.
![]()
CHAPTER 2
PORTABLE CHEST TECHNIQUE IN THE ICU
The portable chest radiograph is the most common test used at the bedside to evaluate the cardiopulmonary status of patients in the ICU. On the portable film, one can detect the positions of lines, tubes, and monitoring devices as well as evaluate the patient’s disease status and response to therapy.1
Careful attention should be given to the technique used in obtaining a chest radiograph. The quality of the portable radiography is often highly variable and generally inferior to examinations performed in the main department. Poor technical quality of a portable chest radiograph may result in a delay or the inability to establish a diagnosis. Because of the portable film’s necessity and its variable quality, it is important for the reader to understand, and keep in mind, several important differences between routine chest films obtained in the x-ray department and those obtained portably.2
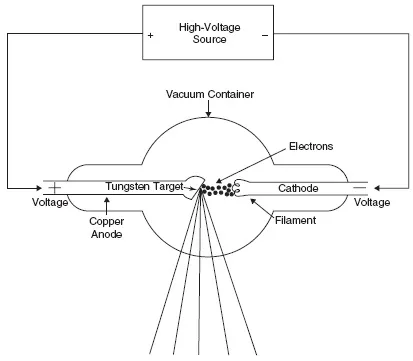
A portable chest radiograph is often of inferior quality because of (1) the difficulty controlling scattered radiation, (2) the wide range of densities that need to be demonstrated on a film, and (3) the inability of critically ill patients to cooperate. Furthermore, the portable machine is one of the most inefficient and technically least advanced pieces of imaging equipment in an x-ray department (Fig. 2.1).3
A team approach is needed to obtain a portable chest radiograph, and the team should include technologists, radiologists, and ICU personnel. There should be close cooperation between ICU nurses, respiratory therapists, and other ICU personnel in assisting the technologist while positioning an unstable patient. They should help remove unnecessary and unwanted tubes and lines from the patient’s chest before taking the film because these can be misinterpreted and thought to be in the heart or lungs. Furthermore, every attempt must be made to obtain the film with the patient upright and at the end of deep inspiration. If the radiograph is obtained in expiration when the patient is supine, the findings can be misleading. Finally, it is imperative that there be rapid communication between the radiologist and the ICU team about the findings seen on a chest radiograph.4
Because the quality of the image often determines the diagnostic information that can be obtained from the radiograph, it is necessary to review the factors affecting the film, such as contrast, noise, and spatial resolution.
Contrast represents the variation of film density between one part of the film and another. Ideally one should obtain a film with the highest contrast throughout, and in the chest x-ray this is generally measured from the darkest area (Dmax), which is the lung, to the lightest, white area (Dmin), which is bone. Contrast is the result of the differences between tissues as an x-ray photon passes through the object. The important parameters are thickness and density of the material through which the x-ray passes and the amount of absorption of the photon that occurs. In the diagnostic radiology range (60-150 KVp) the absorption coefficient has a direct relationship to the atomic number of the tissue through which the photon passes. In this range, the absorption coefficient is related to the cube of the atomic number. Objects with a high atomic number have a different contrast resolution than do objects with a lower atomic number. This permits us to differentiate structures because in the chest x-ray the heart has a different density, and a different atomic number, than the surrounding lung. The ribs and bony structures are made up principally of calcium, which has a higher atomic number than the lung and thus absorbs more of the x-ray beam, and are therefore easily visualized.5
Noise degrades an image. It is generally seen as grainy mottle pattern on the x-ray. This is due to the statistical difference in the number of x-ray photons striking the film in different areas. In some areas, there are insufficient numbers of photons, so only a part of the film is exposed, producing a mottled appearance.
Spatial resolution is the ability of an x-ray to depict closely spaced objects. High spatial resolution produces sharper edges in an object than does low resolution. Image sharpness refers to how sharp the edge of an object is when seen adjacent to other objects.6
The key to optimizing the technical quality of a chest radiograph is to minimize variation in the technical parameters from day to day. One should instruct the technologist to choose the same patient position each day and to keep a written record of the previous successful techniques at each patient’s bedside. The first time a film is obtained on an ICU patient, the technologist should show that film to the ICU radiologist, who will determine if the technique is adequate. If so, this technique should subsequently be used on all follow-up films so that the exposure is similar and changes in the most recent x-ray are due to changes in the patient’s condition, rather than changes induced by differences in radiologic technique.7
It is necessary to keep in mind that portable chest films are performed in the anterior posterior (AP) position, resulting in a 15–20% magnification factor to the cardiac shadow. One should be cautious when making the diagnosis of cardiomegaly on an AP film. Remember that one needs an adequate inspiration (9–10 ribs) to establish that diagnosis.8
Exposure variations constitute one of the main difficulties in portable radiography. Photo-timing devices, used in the main department, are generally not used for bedside films.9 Generally, the
exposure must ...