Beginning with introductory chapters on the localization of disease, diagnostics, and therapeutics, the heart of the book focuses on the full range of respiratory diseases, including nasal disorders, diseases of airways, parenchymal diseases, pleural and mediastinal diseases, and vascular disorders. Each chapter takes a common format with diseases subdivided by etiology into structural, infectious, inflammatory, and neoplastic disorders. Clinical Canine and Feline Respiratory Medicine is a useful tool for students and practitioners engaged in studying, diagnosing, and treating respiratory disease.
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
Clinical Canine and Feline Respiratory Medicine
About this book
Clinical Canine and Feline Respiratory Medicine provides reliable information on the diagnosis and management of respiratory disease in a user-friendly format. With an emphasis on the features of the history and physical examination that aid in efficient diagnostic planning, the book is an accessible, readable resource for optimizing treatment of patients with diseases of the respiratory tract. Offering comprehensive, accessible coverage of respiratory disorders, Clinical Canine and Feline Respiratory Medicine is a useful practice guide and study aid for general practitioners and veterinary students.
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
1
Localization of Disease
Clinical signs that provide clues to the existence of respiratory disease include nasal discharge, cough, respiratory noise, tachypnea, difficulty breathing, or exercise intolerance. The first step toward making a diagnosis requires accurate localization of the anatomic origin of disease within the respiratory tract: the nasal cavity, upper or lower airway, lung parenchyma, or pleural space. This will allow construction of an accurate list of differential diagnoses, will facilitate efficient diagnostic testing, and will allow rational empiric therapy while waiting for test results.
Nasal Discharge
History
Nasal discharge is almost always a sign of local disease within the nasal cavity. One exception is eosinophilic bronchopneumopathy, an inflammatory condition of the lung and airways that can also involve the nasal epithelium. A second exception can be found in the dog or cat with lower respiratory tract disease (usually bacterial pneumonia) that coughs airway material into the nasopharynx, which subsequently drains from the nose. In both situations, animals usually have a combination of cough and nasal discharge. The most common causes of nasal discharge include infectious, inflammatory, and neoplastic disorders as well as dental-related nasal disease and foreign bodies (Table 1.1). Additional clinical signs that can be seen in animals with nasal disease include sneezing or reverse sneezing, pawing or rubbing at the face, noisy breathing or mouth breathing, facial pain, or an unexplained odor near the head.
Table 1.1. Causes of nasal discharge in dogs and cats
| Dog | Cat | |
| Infectious | Canine infectious respiratory disease complexa Aspergillus Penicillium Rhinosporidium | Acute upper respiratory tract disease complexb Cryptococcus Aspergillus |
| Inflammatory | Lymphoplasmacytic rhinitis | Feline chronic rhinosinusitis |
| Neoplastic | Adenocarcinoma Sarcomas Lymphoma | Lymphoma Adenocarcinoma Sarcomas |
| Local | Tooth root abscess Oronasal fistula Trauma Foreign body Nasal or nasopharyngeal polyp | Nasal or nasopharyngeal polyp Tooth root abscess Oronasal fistula Foreign body Trauma |
| Other | Primary ciliary dyskinesia Nasal mites Xeromycteria (dry nose syndrome) | Primary ciliary dyskinesia |
aReported causes include canine adenovirus-2, canine parainfluenza-3 virus, canine respiratory coronavirus, canine herpesvirus, canine distemper virus, Bordetella and Mycoplasma. Canine influenza virus is a new addition to the list of etiologic agents.
bReported causes include feline herpesvirus-1, feline calicivirus, Chlamydophila, Bordetella, and Mycoplasma.
When evaluating the animal with nasal discharge, important considerations include the duration of signs, the type of discharge as well as changes in its character over time, and the presence of unilateral or bilateral signs. Acute nasal discharge is often accompanied by sneezing and is most commonly associated with viral upper respiratory tract disease or a foreign body. Animals with acute nasal discharge usually have dramatic clinical signs that either resolve within a week without treatment or are so severe that animals are rapidly evaluated by a veterinarian. More frustrating cases are those with chronic nasal discharge, which often have low level but progressive signs from weeks to months to years before the severity of disease prompts veterinary care.
With many causes of nasal disease including viral disease or foreign body, discharge is serous initially and then progresses to a mucoid character when inflammation induces mucus production or when secondary bacterial infection develops. Yellow-green nasal discharge can be an indicator of eosinophilic disease but is also encountered in other inflammatory conditions, while brown-tinged discharge suggests the presence of blood within the mucus. Bright red blood can be found in combination with nasal discharge because of trauma to blood vessels associated with the primary disease process or due to the severity of sneezing. Pure epistaxis has been associated with local causes of disease, including inflammatory rhinitis, canine aspergillosis, and neoplasia; however, systemic vascular disorders must also be considered including coagulopathies and systemic hypertension.
Nasal discharge that is strictly unilateral is most suspicious for local disease due to a foreign body, trauma, tooth root abscess or oronasal fistula, or an early fungal infection or neoplasm. However, systemic vascular disease or a coagulopathy can result in unilateral signs. Also, inflammatory diseases such as lymphoplasmacytic rhinitis in the dog and feline chronic rhinosinusitis can also present with lateralizing clinical signs, although in most cases, imaging and histology reveal that both sides of the nasal cavity are affected.
Signalment
Young animals with nasal discharge are most often affected by infectious upper respiratory tract diseases. A nasopharyngeal polyp should be considered when discharge is accompanied by obstructed breathing. Primary ciliary dyskinesia is a defect of innate immunity that results in effectual mucociliary clearance, failure to clear secretions, and recurrent infection. Therefore, this condition would be more frequently recognized in a younger animal. Affected dogs are often purebred, with an increased prevalence in the Bichon Frise, although any breed of dog or cat can be affected. While neoplastic disease most typically affects older animals, it also occurs in animals 2–4 years of age and can be particularly aggressive, especially in dogs. Canine aspergillosis is most often encountered in younger dogs and older cats. Cryptococcus and inflammatory rhinitis can affect dogs or cats of any age.
Nasal disease of most types (fungal, neoplastic, and inflammatory) is most commonly found in dolicocephalic dog breeds. An unusual combination of rhinitis and bronchop-neumonia has been reported in the Irish wolfhound, where a genetic defect in respiratory immunity is suspected.
Physical Examination
A complete physical examination is essential in every animal presented for evaluation of respiratory disease. In animals with nasal discharge, important features to focus on include the presence or absence of nasal airflow, changes in ocular retropulsion, lack of soft palate depression, regional local lymph node enlargement, and facial asymmetry or pain. These parts of the physical examination are most important because they can help identify the space-occupying nature of some nasal diseases, particularly nasal neoplasia, feline cryptococcosis, and nasopharyngeal polyps, and because these findings can detect local extension or metastasis.
Nasal airflow can be assessed by holding a chilled microscope in front of each nostril to show fogging of the glass or by using a wisp of cotton (from a cotton ball or Q-tip) to watch for air movement. The mouth should be held closed during the procedure, and occlusion of the alternate nostril can be helpful for enhancing airflow through the side of the nasal cavity to be examined (Figure 1.1). An animal with a mass effect in the nasal cavity or nasopharynx will fail to fog the glass or move the cotton wisp and will often object to this manipulation because it obstructs airflow. Conversely, even animals with heavy mucus accumulation in the nasal cavity will retain nasal airflow.
Facial palpation is performed to assess for a pain response, to locate swellings and depressions in bony structures, and to check for symmetry of the skull. Ocular retropulsion is a part of the facial examination and is performed by placing each thumb over the closed lids and pressing gently backward, upward, medially, and laterally (Figure 1.2). Nasal lesions that are producing a mass effect behind the globe (primarily a neoplasm or retrobulbar abscess) will cause a lateralizing difference in the resistance to depression. Similarly, palpation within the oral cavity can reveal bony abnormalities in the hard palate or might suggest a mass lesion above the soft palate. To perform this examination, the mouth is held open, and the roof of the mouth is palpated from the front of the hard palate through to the end of the soft palate. In the normal animal, the soft palate is readily depressed upward into the nasopharyngeal region (Figure 1.3). A mass in this area (most commonly a neoplasm, fungal granuloma, or polyp) will resist depression. The dental arcade should also be evaluated during the oral examination, although it is important to remember that tooth root disease can be present in the absence of external signs.
Figure 1.1. Nasal airflow can be assessed by occluding one nostril and assessing flow from the alternate nostril with a cotton wisp or chilled microscope slide.
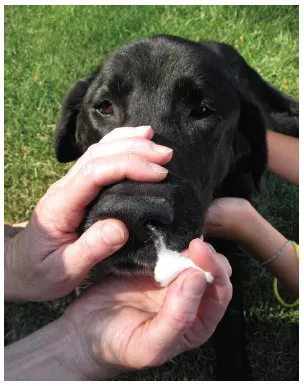
Figure 1.2. Palpation during ocular retropulsion can suggest the presence of a mass lesion within the optic tract.

Figure 1.3. In the normal animal, palpation of the soft palate will readily depress tissue into the nasopharyngeal region. The presence of a mass lesion in the nasopharynx will result in resistance to depression.

Neoplastic disease, fungal infection, or inflammatory diseases within the nasal cavity can involve mandibular lymph nodes and the disease process can sometimes be identified by cytology of a lymph node aspirate, even when there is no palpable enlargement. Nasal depigmentation is a relatively specific feature of canine nasal aspergillosis found in up to 40% of cases and is thought to result from elaboration of a dermonecrotic toxin by the fungus.
Loud Breathing
Definition
Loud breathing most commonly results from a disorder affecting the nasal cavity or upper airway (larynx, pharynx, or cervical trachea), although occasionally animals with lower airway disease will present for loud breathing. Stertor is a gurgling or snoring sound that is produced as air flows past a soft tissue obstruction. It can be caused by narrowing of the nasal cavity, by elongation or thickening of the soft palate, or by edema or eversion of laryngeal saccules. It varies in tone and pitch, and it may be audible on both inspiration and expiration. In contrast, stridor is classically an inspiratory noise of a single, high pitch that results from rapid flow of air past a rigid obstruction, such as a paralyzed or collapsed larynx. Stridor can also be heard in an animal with a laryngeal mass effect, or occasionally in an animal with nasopharyngeal stenosis or fixed cervical tracheal collapse or stenosis.
Signalment
Stertor is commonly encountered in brachycephalic dog breeds such as bulldogs (English and French), Pugs, and Boston Terriers and is also seen in Himalayan and Persian cats. Loud breathing is often present early in life and becomes worse with development of additional respiratory disease or with weight gain. Some animals are not presented for evaluation of stertor and respiratory difficulty until late in life because of the perception that noisy respiration is “normal” for the breed.
Animals with stridor due to congenital laryngeal paralysis are usually young (6–12 weeks) when the disease is manifest. Affected breeds include the Dalmatian, Rottweiler, Great Pyrenees, Bouvier des Flandres, Siberian Husky, White German Shepherd, and some cats (see Chapter 5). Acquired laryngeal paralysis is most commonly found in older large breed dogs such as Labrador and Golden retrievers. Brachycephalic breed dogs that develop laryngeal collapse are usually older at the time of diagnosis, however because this is an end-stage manifestation of airway obstruction, age varies depending on the severity of disease.
Physical Examination
In a normal animal, breathing is quiet at rest. Stertor and stridor can be heard without the use of a stethoscope; however, in some instances, careful auscultation over the neck region is needed to confirm stridor. Increasing respiratory flow rate by gentle exercise can improve detection of stridor; however, panting must be discouraged. In the normal animal, auscultation over the larynx and trachea will reveal loud, hollow sounds that are heard equally on inspiration and expiration. Because upper respiratory noises are typically loud and can obscure lung sounds, auscultation of the larynx and tracheal region is recommended in all patients/prior to thoracic auscultation to improve differentiation of upper from lower respiratory sounds and to improve detection of heart sounds. This is particularly helpful in brachycephalic breeds (Figure 1.4). Brachycephalic breeds commonly have visible stenotic nares as part of the disease complex, and excessive oropharyngeal folds may be evident.
Figure 1.4. Prior to thoracic auscultation, the laryngeal and cervical tracheal regions are ausculted to define upper airway sounds.

Cough
History
Cough occurs because of activation of irritant receptors that lie between epithelial cells lining the airways and can be triggered by inflammatory products of neutrophils or eosinophils, by the presence of excess secretions, and by airway compression or collapse (Table 1.2). Important historical features to determine include the onset and duration of cough, the character of the cough, and environmental features that appear to trigger cough.
Animals with a wet- or moist-sounding cough most likely have excessive airway secretions due to infectious or inflammatory airway or parenchymal disease. Observant owners of the animal with a productive cough may note that the animal swallows after coughing or retches to remove secretions from the airway. However, infectious, inflammatory, and structural diseases of the airway can also result in a dry cough when secretions are minimal or early in the course of disease. Cough in animals with airway disease is often harsh and can be chronic, intermittent, or paroxysmal in nature. Animals with pneumonia may have a softer cough along with a vague history of illness characterized by anorexia and lethargy.
Determining environmental and travel history is important for animals with cough. Exposure to a high-density dog population should raise concern for disease associated with canine respiratory disease complex. If the cough is harsh and dry, Bordetella should be considered, while a soft, chronic cough could be suggestive of canine influenza virus infection. Sporting dogs that develop an acute onset of cough or have a chronic, antibiotic-responsive cough may have foreign body pneumonia. Fungal pneumonia should be suspected in animals with cough that have traveled to endemic regions. In those animals, cough is usually accompanied by tachypnea and systemic signs of illness. Finally, environmental history is important because exposure to pollutants and airway irritants can exacerbate upper or lower airway diseases in both dogs and cats.
Table 1.2. Respiratory causes of cough in dogs and cats
| Dog | Cat | |
| Infectious tracheobronchitis | Canine infectious respiratory disease complexa | Mycoplasma Bordetella |
| Pneumonia | Bacterial Aspiration Foreign body Fungal Eosinophilic... |
Table of contents
- Cover
- Contents
- Title Page
- Copyright
- Dedication
- Preface
- Acknowledgments
- 1 Localization of Disease
- 2 Respiratory Diagnostics
- 3 Respiratory Therapeutics
- 4 Nasal Disorders
- 5 Diseases of Airways
- 6 Parenchymal Disease
- 7 Pleural and Mediastinal Disease
- 8 Vascular Disorders
- Glossary
- Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Clinical Canine and Feline Respiratory Medicine by Lynelle R. Johnson in PDF and/or ePUB format, as well as other popular books in Medicine & Veterinary Medicine. We have over 1.5 million books available in our catalogue for you to explore.