- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
About this book
In the event of a paediatric cardiac arrest, it is essential to be able to respond rapidly, providing safe and effective care. The second edition of this successful text provides nurses with a practical and systematic guide to the rapid assessment and delivery of appropriate resuscitation to infants and children.
- Conforms to current European Resuscitation Council Guidelines
- Based on up-to-date research and evidence-based practice protocols
- Synoptic approach enables rapid delivery of effective treatment
- Written by experts in the field of both resuscitation and paediatrics
Paediatric Advanced Life Support is a succinct yet comprehensive guide and is an essential purchase for any health professional likely to encounter an emergency situation.
Tools to learn more effectively

Saving Books

Keyword Search

Annotating Text

Listen to it instead
Information
Chapter 1
An Overview of Paediatric Advanced Life Support
Introduction
Paediatric advanced life support (PALS) includes the knowledge and skills necessary to identify and effectively treat infants and children who have potential respiratory or circulatory failure, and to provide the appropriate early treatment for a paediatric cardiac arrest.
The aim of this chapter is to provide an overview of PALS.
Learning Objectives
At the end of this chapter, the reader will be able to:
- Discuss the causes of death in childhood
- Discuss survival rates following paediatric resuscitation
- Outline the pathophysiology of paediatric cardiac arrest
- Discuss the importance of treating children differently from adults
- Outline the provision of a resuscitation service in hospital
Causes of Death in Childhood
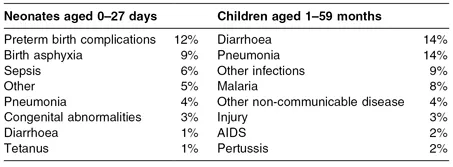
The most common causes of death in children under 6 years of age worldwide are detailed in Table 1.1.
Table 1.1 Most common causes of death worldwide in children under 6 years of age
Reproduced from Stevenson & Tedrow (2010).
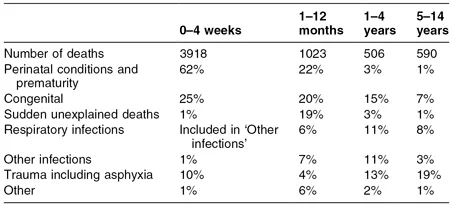
According to the Office for National Statistics (2009), the highest death rates in childhood occur during the first year of life, particularly the first month (Table 1.2). Causes of death in childhood vary according to age. The most common causes are:
- Newborn period – congenital abnormalities and factors associated with prematurity
- 1 month to 1 year – cot death, infection and congenital abnormality
- From 1 year – trauma
Table 1.2 Causes of death by age in England and Wales, 2008
Reproduced from Office for National Statistics (2010).
In England and Wales, infant mortality rates (number of deaths of children under 1 year of age in one calendar year per 1000 live births in the same calendar year) have fallen by more than 50% in the last 28 years, from 12 in 1980 down to 4.5 in 2008, the lowest on record (Advanced Life Support Group, 2011).
Survival Rates Following Paediatric Resuscitation
Paediatric cardiac arrest is rarely caused by a primary cardiac problem. It is also rarely a sudden event (Klitzener, 1995), often being the end result of a progressive deterioration in respiratory and circulatory function (American Academy of Paediatrics, 2000). If cardiac arrest ensues, the prognosis is dismal (O’Rourke, 1986); the survival rate of patients in asystole has been reported to be as low as 3% (Zaritsky et al., 1987).
The early diagnosis and aggressive management of respiratory or cardiac insufficiency aimed at preventing deterioration to cardiac arrest are the key to improving survival without neurological deficit in seriously ill children (Zideman & Spearpoint, 1999). Prompt resuscitation in the event of a respiratory arrest is associated with a favourable outcome – survival rates of over 50% have been reported (Zaritsky et al., 1987; Spearpoint, 2002). Recognition of respiratory failure and shock is discussed in Chapter 3.
Pathophysiology of Cardiac Arrest
There are three basic mechanisms of paediatric cardiac arrest – asystole, pulseless electrical activity (PEA; formerly known as electromechanical dissociation) and ventricular fibrillation (VF). Pulseless ventricular tachycardia (VT) is another mechanism, but this is usually classified with VF because the causes and treatment are similar.
Asystole
Asystole (Fig. 1.1) is the most common presenting rhythm in paediatric cardiac arrests (Sirbaugh et al., 1999; Young & Seidel, 1999). It is the final common pathway of respiratory or circulatory failure (Zideman, 1997). Prolonged severe hypoxia and acidosis leads to progressive bradycardia and asystole (Advanced Life Support Group, 2011). The most common cause is hypoxia, and the most effective treatment is to establish a clear airway and effective ventilation (Zideman, 1997).
Fig. 1.1 Non-shockable rhythm: asystole.

Management of asystole is less commonly successful than when the rhythm is VF (Dieckmann & Vardis, 1995), but survival to discharge has been reported (Spearpoint, 2002).
Pulseless Electrical Activity
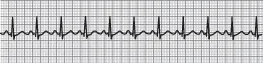
‘Pulseless electrical activity’ is a term used to signify the features of cardiac arrest associated with a normal (or near-normal) ECG (Fig. 1.2). The diagnosis is made on clinical grounds by the combination of the absence of a cardiac output with a ECG rhythm on the monitor that would normally be associated with a good cardiac output.
Fig. 1.2 Non-shockable rhythm: pulseless electrical activity.
The causes of PEA can be classified into one of two broad categories:
- Primary PEA – there is failure of excitation contraction coupling in the cardiac myocytes resulting in a profound loss of cardiac output. Causes include hypoxia, poisoning, for example due to beta-blockers, calcium channel blockers or toxins, and electrolyte disturbance (hyperkalaemia or hypocalcaemia).
- Secondary PEA – there is a mechanical barrier to ventricular filling or ejection. Causes include hypovolaemia, cardiac tamponade and tension pneumothorax.
In all cases, treatment is directed towards the cause.
Ventricular Fibrillation/Pulseless Ventricular Tachycardia
VF/pulseless VT (Fig. 1.3) is uncommon in children (Zideman, 1997; Spearpoint, 2002). However, clinical situations when it may occur include after cardiac surgery or with cardiomyopathy, congenital heart disease, hypothermia or drug intoxication.
Fig. 1.3 Shockable rhythms: ventricular fibrillation (a) and pulseless ventricular tachycardia (b).
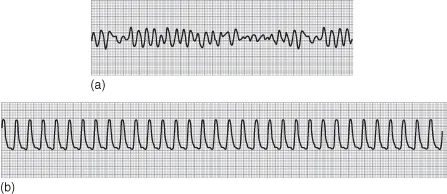
The ECG displays a bizarre irregular waveform, apparently random in both frequency and amplitude, which reflects disorganised electrical activity in the myocardium. This is an eminently treatable arrhythmia, but the only effective treatment is early defibrillation, and the likelihood of success is crucially time-dependent (Jevon, 2009).
Conditions for defibrillation are optimal for as little as 90 seconds after the onset of the rhythm, and the chances of success fall by about 10% with every minute that treatment is delayed (Waalewijn et al., 2001). Untreated VF will inevitably deteriorate into asystole as myocardial energy reserves and oxygen are exhausted; successful cardiopulmonary resuscitation (CPR) at this late stage is almost impossible (Waalewijn et al., 2001).
Importance of Treating Children Differently from Adults
Children are not small adults. Children are a diverse group of the population. They vary dramatically in weight, size, shape, intellectual ability and emotional responses.
At birth, a child is, on average, 3.5 kg, with a small respiratory and cardiovascular reserve and an immature immune system. At this stage, children are capable of limited movement, exhibit limited emotional responses and are dependent upon adults for their needs. Fourteen or more years later, at the other end of ch...
Table of contents
- Cover
- Title page
- Copyright page
- Foreword
- Contributors
- Chapter 1 An Overview of Paediatric Advanced Life Support
- Chapter 2 Resuscitation Equipment for Paediatric Resuscitation
- Chapter 3 Recognition of the Seriously Ill Child
- Chapter 4 Paediatric Basic Life Support
- Chapter 5 Airway Management and Ventilation
- Chapter 6 ECG Recognition and Management of Cardiac Arrhythmias
- Chapter 7 Defibrillation and Electrical Cardioversion
- Chapter 8 Paediatric Advanced Life Support
- Chapter 9 Management of Anaphylaxis
- Chapter 10 Resuscitation in Special Situations
- Chapter 11 Post-resuscitation Care
- Chapter 12 Bereavement
- Chapter 13 Records, Record-keeping and Audit
- Chapter 14 Legal and Ethical Issues
- Chapter 15 Resuscitation Training
- Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.4M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Paediatric Advanced Life Support by Philip Jevon in PDF and/or ePUB format, as well as other popular books in Medicine & Pedriatic Nursing. We have over one million books available in our catalogue for you to explore.