![]()
Part 1
General Introduction to Hypertension
Hypertension Prevalence and Consequences
Hypertension is one of the major risk factors for coronary heart disease (CHD), myocardial infarction (MI), cerebrovascular accidents (CVA), chronic renal failure (CRF), and congestive heart failure (CHF) in the United States and in westernized or industrialized countries around the world. In industrialized countries, the risk of becoming hypertensive (blood pressure [BP] >140/90 mm Hg) over a lifetime is >90%. CHD is the leading cause of death in the United States, accounting for more than 800 000 deaths per year (more than one death per minute), and CVA is the fourth leading cause of death in the United States.
The annual expenditure for CHD is over 200 billion dollars [1–3]. Essential hypertension is defined as an increase in BP of unknown cause that increases the risk for cardiovascular (CV) diseases such as cerebral, cardiac, large artery, and renal events. However, subclinical vascular target organ damage (TOD) occurs very early in the course of hypertension and can be identified with noninvasive testing. These subtle CV findings include left ventricular hypertrophy (LVH), diastolic dysfunction, microalbuminuria, abnormal vascular compliance, and abnormal cognitive dysfunction or vascular dementia.
Hypertension Syndrome
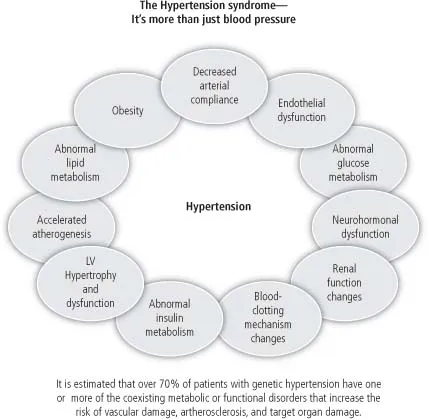
Hypertension is a part of heterogeneous condition that is best described as an atherosclerotic syndrome or hypertension syndrome with genetic and acquired structural and metabolic disorders (Figure 1) including the following [4, 5, 147]:
1. Dyslipidemia or hyperlipidemia
2. Insulin resistance, impaired glucose tolerance, and diabetes mellitus (DM)
3. Central obesity (android or portal obesity)
4. Endocrine and neurohormonal changes (sympathetic nervous system [SNS], Renin-Angiotensin-Aldosterone System [RAAS])
5. Renal function abnormalities (sodium, water, uric acid, protein load excretion, and microalbuminuria)
6. Abnormalities of vascular and cardiac smooth muscle structure and function such as arterial compliance abnormalities with loss of arterial elasticity, diastolic dysfunction, and LVH.
7. Membranopathy and abnormal cellular cation transport (Ca++, Mg+, Na+, and K+)
8. Abnormalities of coagulation (prothrombotic)
9. Endothelial dysfunction
10. Vascular inflammation (high sensitivity C-reactive protein [HS-CRP])
11. Aging
12. Accelerated atherogenesis
Subsets of Hypertension Approach to Treatment
By definition, all antihypertensive drugs lower BP, which is clearly the most important determinant for the reduction of CV risk. However, differences exist among the various antihypertensive drug classes, as well as within the same class, with respect to target organ disease and prevention of major CV events. The majority of hypertensive patients will require two or more drugs to reach newer BP goals, and those hypertensive patients with high risk for CV disease will need concomitant statin use as well to maximize CV risk reduction. However, despite effective drug for hypertension, the majority of patients around the world remain uncontrolled, with the United States having the best overall BP control.
The clinician seeking optimal antihypertensive drug therapy must recognize a myriad of new challenges and concepts. Individualization of treatment is recommended on the basis of the subsets of hypertension approach [5]. An essential component of individualized treatment is a logical and tailored selection of drug therapies based on:
1. Pathophysiology and vascular biology
2. Renin and aldosterone profiling
3. Hemodynamics
4. Risk factor reduction and end-organ damage reduction
5. Concomitant medical diseases or problems
6. Demographics
7. Quality of life (QOL) and adverse effects of treatment
8. Compliance with therapy
9. Total health care cost
This will be discussed in detail in the following chapters.
Clinical Hypertension Trials: A Perspective
This first edition of The Hypertension Handbook includes many new concepts, changes in philosophy, clinical information, clinical trials, new antihypertensive drugs, and nonpharmacological treatment. Large-scale clinical trials comparing the older antihypertensive drug regimens with newer agents have been completed, and many others are in progress. The recently published studies include Antihypertensive Therapy and Lipid Lowering Heart Attack Prevention Trial (ALLHAT), Anglo-Scandinavian Cardiac Outcomes Trial (ASCOT), TROPHY, International Nifedipine GITS Study: Intervention as a Goal in Hypertension Trial (INSIGHT), Nordic Diltiazem Study (NORDIL), Losartan Intervention For Endpoint reduction in hypertension (LIFE), African American Study of Kidney Disease and Hypertension (AASK), Randomized Evaluation of NIDDM with the Ang-II antagonist Losartan (RENAAL), Irbesartan Diabetes Nephropathy Trial (IDNT), IRMA, Controlled Onset Verapamil Investigation of Cardiovascular Endpoints (CONVINCE), ANBP-2, Valsartan Antihypertensive Long-Term Use Evaluation (VALUE), JIKEI, and MOSES.
The Systolic Hypertension Trial in Europe (SYST-EUR), Shanghai Trial of Nifedipine in the Elderly (STONE), Systolic Hypertension in China (SYST-CHINA), Hypertension Optimal Treatment (HOT), and the Chen-Du Nifedipine Trial, INSIGHT, NORDIL, NIC-EH, CONVINCE, Prospective Randomized Evaluation of Vascular Effects of Norvasc Trial (PREVENT), Verapamil in Hypertension and Atherosclerosis Study (VHAS), Study Group on Long-term Antihypertensive Therapy (GLANT), Practitioners Trial on the Efficacy of Antihypertensive Treatment in the Elderly (PATE), Swedish Trial in Old Patients–2 (STOP-2), VALUE, ALLHAT, and ASCOT have documented significant reductions in CV and cerebrovascular morbidity and mortality with calcium channel blockers (CCBs), especially the dihydropyridine CCBs.
The Captopril Prevention Project (CAPPP) and ANBP-2 showed that angiotensin- converting enzyme inhibitors (ACEIs) reduce CV morbidity and mortality in hypertensive patients equal to or better than conventional diuretic and beta- blocker (BB) therapy. The Heart Outcomes Evaluation (HOPE) and EUROPA studies showed that ACEIs reduced CV death in a high-risk nonhypertensive population.
The treatment of the hypertensive patient with DM with proteinuria has now been shown in SYST-EUR, CAPPP, RENAAL, IDNT, IRMA, LIFE, VALUE, and ASCOT to be better with ACEIs, Angiotensin receptor blockers (ARBs), and CCBs than with conventional diuretic or BB therapy in reducing CV morbidity and mortality.
The STOP-2 showed that calcium blockers and ACEIs are equal to conventional therapy in reducing CV morbidity and mortality and superior in reducing CVA and equal BP levels. The PROGRESS trial, STOP-2, MICROHOPE, QUIET, SCAT, AASK, Appropriate Blood Pressure Control in Diabetes Trial (ABCD), ALLHAT, Fosinopril and Amlodipine Cardiac Events Trial (FACET), GLANT, ANBP-2, and PATE have proven significant reductions in CV morbidity and mortality with ACE...