eBook - ePub
Anesthesia and the Fetus
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
Anesthesia and the Fetus
About this book
Anesthesia and the Fetus integrates into one volume the multidisciplinary components of:
- fetal development
- fetal pharmacology
- assessments of fetal and neonatal outcome
- anesthesia and analgesia during pregnancy
- anesthesia and analgesia during labor
- ethics and law
Written by an internationally renowned group of clinicians and scientists, Anesthesia and the Fetus provides a contemporary guide and reference to the role of anesthesia, and the anesthesiologist, in protecting the mother and her unborn child during pregnancy.
Tools to learn more effectively

Saving Books

Keyword Search

Annotating Text

Listen to it instead
Information
Basic Principles
1
Intrauterine Growth and Development
Introduction
The birth of a healthy, full-term infant is the result of the successful orchestration of a multitude of individual developmental events. These processes are affected by genetic and environmental influences starting before conception and extending throughout gestation. Congenital abnormalities, which are present in up to 5% of human births, usually result from abnormalities in very early development. For example, many organ systems form between four and eight weeks after fertilization (Table 1.1), making them particularly vulnerable to teratogenic exposure during this period. The majority of congenital abnormalities can be detected in utero by routine ultrasound imaging [1]. For those that may be fatal to the fetus or neonate or result in severe life-long disability, the option of fetal surgical intervention is becoming increasingly possible [2]. However, the widespread adoption of fetal interventions for prenatal correction of congenital abnormalities has not yet been established and most techniques are currently experimental [2, 3]. By far the greatest obstacle to successful outcomes after fetal interventions is preterm birth and its associated complications [3].
Table 1.1 Timing of structural and functional development of major organs.
| Organ | Anatomical origin | Onset of function |
| Adrenals | The adrenal cortex arises from mesenchymal cells (mesoderm), superior to the developing gonads, at 6 weeks. The adrenal medulla is formed from an adjacent sympathetic ganglion (ectoderm) during the eighth week. | Dihydroepiandosterone sulfate is synthesized at 6–8 weeks. Cortisol is produced from progesterone at 8–12 weeks. |
| Heart | The angioblastic cords, which arise from splanchnic mesenchyme (mesoderm) fuse to form the primitive endothelial heart tube at ∼22 days. Folding of the heart tube and septation to form left and right atria and ventricles are complete by 8 weeks. | Myogenic contractions first begin on day 21–22. Coordinated contractions resulting in forward flow occur by 4 weeks. The conducting system of the heart originates with the formation of the sinoatrial node during the fifth week. |
| Lungs | The lower respiratory tract begins as the laryngotracheal tube by budding of endoderm, into the surrounding splanchnic mesenchyme, from the ventral primitive foregut during weeks 4–5. Bronchial buds form and progressively branch to form the conducting and respiratory regions of the lungs. Lung structural development (airway branching and alveolarization) continues until after birth. | The fetal lungs actively secrete fluid that expands the lungs, which is critical for normal lung growth. Clearance of lung liquid at birth allows the initiation of gas exchange. Production of pulmonary surfactant, which is critical for lung function after birth, is initiated at ∼24 weeks. |
| Kidneys | After the pronephroi and mesonephroi, the metanephroi develop during the 5th week as the ureteric bud penetrates metanephric mesoderm. Ureteric bud branching forms the renal tubules, which are invaginated by glomeruli to form nephrons (the functional unit of the kidney). Nephrogenesis is complete before full term. | Glomerular filtration begins at approximately the 9th week. The fetal kidneys produce copious dilute urine, which provides the majority of amniotic fluid volume. |
| Gonads | Sexual differentiation of the gonads does not occur until the seventh week after fertilization. The undifferentiated gonads arise from mesodermal epithelium and underlying mesenchyme, medial to the mesonephros, during the 5th week to form the gonadal ridges. Primary sex chords (of epithelial origin) then penetrate the underlying mesenchyme. The undifferentiated gonads consist of an epithelial cortex and mesenchymal medulla by 6 weeks. Primordial germ cells, present in the yolk sac endoderm early in the 4th week, migrate to the primary sex chords during the 6th week. | |
| Testis | Under the influence of the SRY gene, the primary sex chords develop into extended and anastomosed seminiferous tubules at approximately 7 weeks. The epithelial cells of the tubules give rise to the sertoli cells; spermatogonia arise from the primordial germ cells. | Testosterone production by the developing testis begins at ∼8 weeks. Spermatogenesis does not occur until puberty. |
| Ovaries | The ovaries are first apparent at ∼10 weeks. The primary sex cords degenerate and secondary sex chords develop from the cortical epithelium to form primordial follicles at ∼12 weeks, which contain oogonia, differentiated from primordial germ cells, surrounded by follicular cells derived from the secondary sex chords. | Ovarian steroidogenesis begins after the 28th week of gestation. Ovulation does not occur until puberty. |
| Brain | The nervous system arises from the neural folds (ectoderm) on the dorsal surface of the embryonic disc at ∼3 weeks. During week 4 the prosencephalon, mesencephalon (which gives rise to the midbrain and superior and inferior colliculi), and rhombencephalon (demarcated from the spinal cord by the cervical flexure) form. During the 5th week the prosencephalon gives rise to the telencephalon (which gives rise to the cerebral cortex and basal nuclei) and diencephalon (which forms the retina, thalamus, and hypothalamus); the metencephalon (which forms the pons and cerebellum) and myelencephalon (which becomes the medulla) form from the rhombencephalon. | Disorganized neural activity is likely to be present from 5–6 weeks. Synapses do not form substantially until 17 weeks and peak later in gestation, continuing postnatally (in combination with synaptic pruning). Fetal responsiveness indicative of higher brain function does not occur until the second half of gestation. Fetal behavioural (sleep) states are indirectly identifiable (based on the presence of rapid eye movements) at 28–31 weeks. |
| Liver | The liver forms from a ventral outgrowth of the foregut in the fourth week. | Hematopoiesis begins in the liver during the 6th week. Bile formation begins during the 12th week. |
| Spleen | The spleen begins to develop during the 5th week, from mesenchymal cells in the dorsal mesentery. The splenic circulation is established during weeks 6–7. | Lymphoid colonization of the spleen begins during week 18. |
| Pancreas | The pancreas originates as two buds from the developing duodenum (endoderm) within the ventral mesentery during the 5th week. These buds fuse and their separate ducts anastomose during gut rotation. | Insulin secretion begins in the 10th week. |
| Pituitary | Ectoderm of oral origin begins to form the adenohypophysis of the pituitary (pars tuberalis, pars distalis, pars intermedia) at the beginning of the 4th week. At this stage the neurohypophysis (median eminence, infundibular stem, pars nervosa) begins to form as an infundibulum of the diencephalon. | Adrenocorticotrophic hormone (ACTH) is released by the pituitary by 8 weeks. |
| Thyroid | The thyroid develops at ∼24 days from endoderm at the base of the primitive pharynx and attains its adult appearance and anatomical location by 7 weeks. | Thyroid hormone production begins at 10–12 weeks. |
| Thymus | The thymus develops from epithelial cells (endoderm) of the third pharyngeal pouch, which penetrate the surrounding mesenchyme (which later forms thin septae between thymic lobules). T cell progenitors (hematopoietic stem cells) begin to populate the thymus from 7 weeks. | Mature T cells are evident in the fetal thymus from 8 weeks. |
| Gastrointestinal tract | During the 4th week, the primitive foregut arises when embryonic folding incorporates the dorsal part of the yolk sac into the embryo. The digestive tract epithelium and glands arise from endoderm and the layers of the wall of the digestive tract are derived from the surrounding splanchnic mesenchyme; ectoderm gives rise to oral and anal epithelia. | Meconium appears in the small bowel during the 14th week and accumulates in the colon from 18 weeks. Some gastrointestinal hormones are secreted from as early as 8 weeks. |
In this chapter, we summarize the current understanding of processes involved in implantation and organogenesis, the major developmental abnormalities that are amenable to surgical intervention during gestation and/or delivery, development of the fetus, and factors that affect its growth and development.
Early Development and Placentation
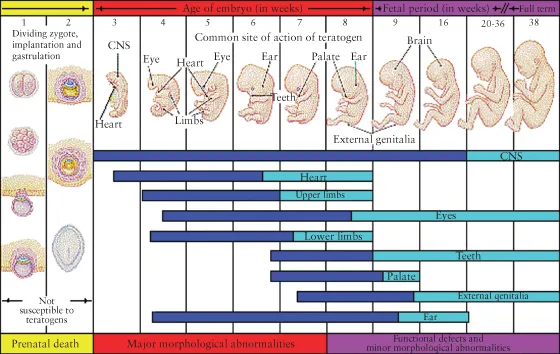
Human development begins with the formation of the zygote soon after fertilization. Initial zygotic cleavage results in two cells (blastomeres), which undergo further divisions (cleavage) within the zona pellucida surrounding the zygote. Cleavage occurs without an increase in cytoplasmic mass, so each division results in successively smaller blastomeres. The blastomeres are compacted to form the morula within four days of fertilization. Fluid spaces within the morula then coalesce to form the blastocyst cavity, marking the formation of the blastocyst. This coincides with differentiation of the inner cell mass (which will ultimately form the embryo), located at the embryonic pole, from the trophoblast (which makes up the wall of the blastocyst) and degradation of the zona pellucida (Figure 1.1).
Fig. 1.1 Schematic illustration of critical periods of development before birth, showing the timing of vulnerability to teratogens. Highly sensitive periods for organs and systems are shown in dark shading; less sensitive periods are shown in light shading.
Reproduced from Moore K, Persaud TVN, editors. The Developing Human: Clinically Oriented Embryology. 8th edn. Philadelphia: Saunders; 2008. P. 473 with permission from Elsevier.
About one week after fertilization, the embryonic pole of the blastocyst attaches to the uterine endometrial epithelium. The trophoblast cells differentiate into an inner cytotrophoblast layer and an outer syncytiotrophoblast, which begins to invade the endometrium and erode maternal capillaries and venules. Lacunae then form, containing maternal blood and endometrial gland secretions. Secretions of the endometrial glands support the growth of the embryo during the first trimester, resulting in uniform autonomous growth despite potentially very different maternal environments between individual pregnancies [4]. During this period, organogenesis progresses in a low oxygen environment, protected from the potentially mutagenic effects of oxygen free radicals [4].
Normal placentation is dependent on the low oxygen levels present at this time and the privileged immune environment that acts to protect the conceptus from maternal rejection [4, 5]. As the lacunar network increases in volume, maternal arteries in the endometrium begin to contribute to the developing placental circulation and tissue oxygen levels begin to rise. The anatomical relationships between the maternal circulation and invading embryonic tissues, necessary for exchange, are established by the end of the third week after fertilization.
At the end of the second week after fertilization, chorionic villi form from the cytotrophoblast over the entire chor...
Table of contents
- Cover
- Dedication
- Title page
- Copyright page
- Contributors
- Preface
- Acknowledgments
- SECTION 1: Basic Principles
- SECTION 2: Endpoint Variables: Assessments of Fetal Wellbeing and Neonatal Outcome
- SECTION 3: Interventions: Anesthesia, Analgesia, and Their Effects on the Fetus
- SECTION 4: Confounding Variables: The Compromised Fetus, the Compromised Mother
- SECTION 5: Trauma and Resuscitation
- SECTION 6: Medicine, Ethics, and the Law
- Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.4M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Anesthesia and the Fetus by Yehuda Ginosar, Felicity Reynolds, Stephen H. Halpern, Carl Weiner, Yehuda Ginosar,Felicity Reynolds,Stephen H. Halpern,Carl Weiner in PDF and/or ePUB format, as well as other popular books in Medicina & Infermieristica. We have over one million books available in our catalogue for you to explore.