eBook - ePub
Value by Design
Developing Clinical Microsystems to Achieve Organizational Excellence
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
Value by Design
Developing Clinical Microsystems to Achieve Organizational Excellence
About this book
Value by Design is a practical guide for real-world improvement in clinical microsystems. Clinical microsystem theory, as implemented by the Institute for Healthcare Improvement and health care organizations nationally and internationally, is the foundation of high-performing front line health care teams who achieve exceptional quality and value. These authors combine theory and principles to create a strategic framework and field-tested tools to assess and improve systems of care. Their approach links patients, families, health care professionals and strategic organizational goals at all levels of the organization: micro, meso and macrosystem levels to achieve the ultimate quality and value a health care system is capable of offering.
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
CHAPTER 1
INTRODUCING CLINICAL MICROSYSTEMS
LEARNING OBJECTIVES
- Introduce the theory and contexts for microsystems in health care.
- Discuss ways microsystems function in a health care system.
- Summarize important research on microsystems in health care.
- Describe concepts and mechanisms for improving quality and value in clinical practice.
This chapter begins with a sharp focus on clinical microsystems in health care and then expands its focus to explore contexts for microsystems within the overall health care system. After summarizing some important research on microsystems, the chapter concludes with a discussion on essential elements for making sustainable improvements in the quality and value of health care.
MICROSYSTEMS IN HEALTH CARE
There was a time when health care was a simpler affair. The doctor-heroes of such classic television programs as Marcus Welby, M.D. or The Cosby Show modeled practice styles we could recognize in our own personal physicians. Omniscient clinicians delivered care in patients’ homes or in a solo office. Unhurried nurses met every clinical need in hospital settings. Health care was embodied in an intimate one-to-one relationship that joined patient with doctor or nurse and that was supported by relatively little medical science. We developed and maintained a romantic view that health care was a professional activity for heroic soloists.1,2
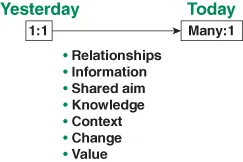
Today, however, that activity, those participants and relationships, and indeed the very goals of health care are much more complex. An interdisciplinary team of clinicians and staff backed up by ancillary services and information technology work in partnership with patient and family members to promote health and to care for health problems. Participants draw upon medical science and biomedical technology that expands at an astonishing (and sometimes overwhelming) rate. Diverse clinical settings with specialized resources, but also unique safety hazards, provide numerous settings in which care may be delivered. Regulators, payers, and consumers all have vested interests in quality performance data that are increasingly available for public review. Health care today has grown, for the most part, into a many-to-one relationship as shown in Figure 1.1, where “many” refers to health care professionals and “one” refers to the patient. Health care is now supported by rapidly proliferating biomedical knowledge, expensive technology, and administrative infrastructure.
FIGURE 1.1 Many-to-One Diagram.
And yet, if we look again at the sharp end of the health care system, at the place where each patient is in direct contact with health care professionals, we can discern the fundamental building block that remains the foundation of all health care systems. We call this building block the clinical microsystem. Clinical reflects the essential priorities of health and care giving. Micro reflects the smallest replicable unit of health care delivery. System reflects that this frontline unit has an aim and is composed of people, processes, technologies, and patterns of information that interact and dynamically transform one another. The clinical microsystem is the place where patients, families, and caregivers meet. It is the locus of value creation in health care.
The theoretical and empirical foundation of clinical microsystem ideas rests upon many decades of pioneering work by such authors as W. Edwards Deming,3 Kerr White,4 Avedis Donabedian,5 and others. But one person in particular, James Brian Quinn, can be regarded as the father of clinical microsystem thinking. Professor Quinn, now Emeritus at Dartmouth’s Tuck School of Business, conducted research in the early 1990s on the economy’s rapidly growing service sector. Quinn wished to understand why some service organizations enjoyed such explosive financial growth and also received accolades from consumers. His research of the world’s best of the best service organizations culminated in publication of the seminal work, Intelligent Enterprise.6 Quinn discovered the world’s most successful service organizations placed a major focus on what he called the smallest replicable units (SRUs) or minimum replicable units (MRUs) within their enterprise. These were the places where true value transfer took place, where suppliers interacted directly with the customers, and where service was delivered.
Quinn found the highest performing service organizations had several features in common, including the following:
- The front office was fixated on the ongoing perfection of frontline services within SRUs because value and loyalty are created at the customer-provider interface.
- Quality, efficiency, timeliness, service excellence, and innovation were designed into frontline work processes of SRUs.
- Information flows were engineered into frontline work of SRUs to create supportive, real-time information environments that facilitated swift and correct delivery of services.
- The smallest units of activity within frontline SRUs were measured and tracked over time for monitoring, managing, and improving performance.
- Increasingly rich information environments were created for the frontline SRUs. Data systems were designed to feed information forward and to feed information back so the right information was at the right place at the right time at the right level of aggregation.
- Based on systemic learning, ongoing improvements, and standardization of most effective practices, these best in the world service sector leaders could rapidly grow by replicating frontline SRUs through time and across space, reliably extending the delivery of high-value services.
The authors of this text, after reading Quinn’s important book, recognized the relevance and prescience of the SRU concept for health care systems. These SRUs, these discrete points of services that unite supplier with customer, are precisely the points that also unite health professionals with patients. The clinical microsystem is the smallest replicable unit of health care. Services are provided or received, and quality, safety, and value are created in microsystems. In this chapter we explore general features of the clinical microsystem, which include its properties, contexts, and empirical supports. In subsequent chapters we examine specific microsystem components that support its optimal function as a self-contained clinical unit and as a building block for larger (macrosystem) health care organizations.
The Functional Unit in Health Care
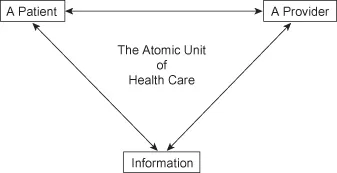
Although far-reaching in its practical implications, the notion of a functional unit in health care is neither a new nor a radical idea. As long ago as 1935, Dr. Lawrence J. Henderson, who more famously described the Henderson-Hasselbalch acid-base equation taught to chemists, physiologists, and medical students, observed in The New England Journal of Medicine that “doctors and patients are part of the same system.”7 More recently, Dr. Staffan Lindblad from the Karolinska Institute in Stockholm, Sweden, has asserted that the clinical microsystem is the atomic unit of all health care systems and it is composed of three particles (P2I), a Provider, a Patient, and Information, all of which dynamically interact with one another over brief or extended periods of time.8 These elements form a system when there is an aim that makes their interdependencies sensible. Figure 1.2 depicts the microsystem as the atomic unit of health care delivery.
FIGURE 1.2 The Simplest Clinical Microsystem.
Source: Adapted from Staffan Lindblad, MD, September 2007.
We have already described the clinical microsystem as the place where patients, families, and caregivers meet. A more formal definition is now useful.
- A health care clinical microsystem is the small group of people (including health professionals and care-receiving patients and their families) who work together in a defined setting on a regular basis (or as needed) to create care for discrete subpopulations of patients. As a functioning unit it has clinical and business aims, linked processes, a shared information and technology environment, and produces care and services that can be measured as performance outcomes. The clinical microsystem evolves over time and is often embedded in larger systems or organizations. As a living, complex, adaptive system, the microsystem has many functions, which include (1) to do the work associated with core aims, (2) to meet member needs, and (3) to maintain itself over time as a functioning clinical unit.9
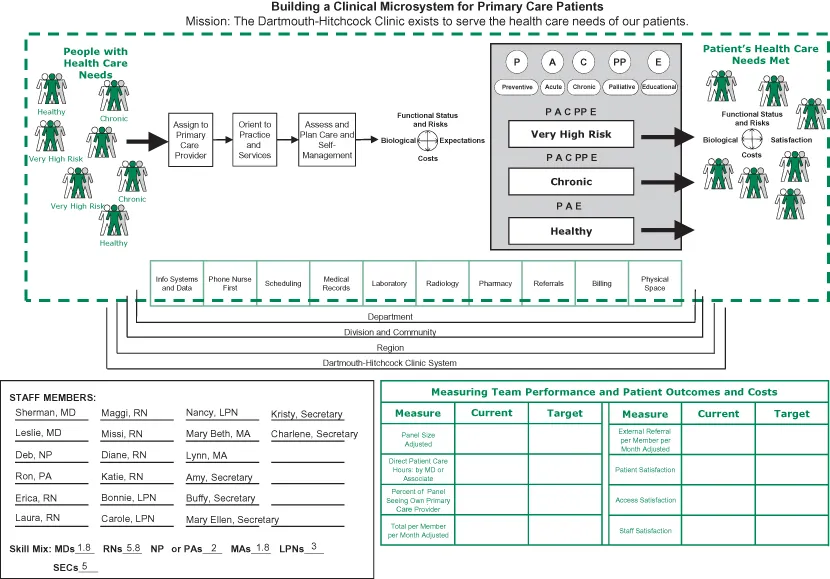
Zimmerman and colleagues have observed that every complex, adaptive system has structure, processes, patterns, and outcomes.10 To the extent that we recognize clinical microsystems as living and dynamic entities of this sort, we can also describe and assess them in terms of both structure (or anatomy) and function (or physiology). The anatomy of the clinical microsystem highlights its major structural elements, including its Purpose, Patients, Professionals, Processes, and Patterns, which together are known as the 5Ps. To design, implement, and improve frontline clinical services, members of clinical microsystems must first gain self-understanding of their own system’s 5Ps. Figure 1.3 depicts structural (anatomical) relationships.
FIGURE 1.3 Anatomy of a Microsystem.
Similarly, caregivers’ rich knowledge of the physiology of the microsystem permits detailed exploration of care processes’ functional inputs and outputs. Patients and families enter a system of care with specific health needs; they participate in clinical processes of orientation, assessment, intervention, and reevaluation; and they hopefully emerge from that system satisfied that their health needs have been met. The physiology model is introduced in the Preface as the Clinical Microsystem Model, Figure P.1.
The elements of the anatomy and physiology models offer powerful insights into systematic assessment of clinical microsystem performance, and they enable formulation of sound recommendations for improvement and innovation. Chapter One Action Guide provides the diagram of the anatomy model with detailed description and useful tools for self-assessment of the 5Ps, and the reader is encouraged to use this resource on a frequent basis when engaged in microsystem design and improvement. In addition, the Web site www.clin...
Table of contents
- Cover
- Half title page
- Title page
- Copyright page
- FIGURES AND TABLES
- FOREWORD
- PREFACE: IMPROVEMENT AT THE FRONT LINE OF CARE
- ACKNOWLEDGMENTS
- THE EDITORS
- THE CONTRIBUTORS
- CHAPTER 1 INTRODUCING CLINICAL MICROSYSTEMS
- CHAPTER 2 PARTNERING WITH PATIENTS TO DESIGN AND IMPROVE CARE
- CHAPTER 3 IMPROVING SAFETY AND ANTICIPATING HAZARDS IN CLINICAL MICROSYSTEMS
- CHAPTER 4 USING MEASUREMENT TO IMPROVE HEALTH CARE VALUE
- CHAPTER 5 STARTING THE PATIENT’S CARE IN CLINICAL MICROSYSTEMS
- CHAPTER 6 DESIGNING PREVENTIVE CARE TO IMPROVE HEALTH
- CHAPTER 7 PLANNING FOR RESPONSIVE AND RELIABLE ACUTE CARE
- CHAPTER 8 ENGAGING COMPLEXITY IN CHRONIC ILLNESS CARE
- CHAPTER 9 SUPPORTING PATIENTS AND FAMILIES THROUGH PALLIATIVE CARE
- CHAPTER 10 DESIGNING HEALTH SYSTEMS TO IMPROVE VALUE
- Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Value by Design by Eugene C. Nelson,Paul B. Batalden,Marjorie M. Godfrey,Joel S. Lazar,Joel S. Lazar in PDF and/or ePUB format, as well as other popular books in Medicine & Public Health, Administration & Care. We have over 1.5 million books available in our catalogue for you to explore.