- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
Prosthodontics at a Glance
About this book
Prosthodontics at a Glance is a title in the popular At A Glance series and focuses on prosthodontics from diagnostics through treatment to post-operative maintenance. It is an ideal companion for all students of dentistry, clinicians and members of the dental team with an interest in prosthodontics.
Tools to learn more effectively

Saving Books

Keyword Search

Annotating Text

Listen to it instead
Information
1
Overview: Rehabilitation of Natural Teeth
An indirect restoration requires taking an impression and employing a dental laboratory to fabricate the prosthesis. Conversely, a direct restoration is carried out chair-side, usually in a single visit, without using a dental laboratory. Dental prostheses can either be intra- or extracoronal.
Indirect Intracoronal Prostheses
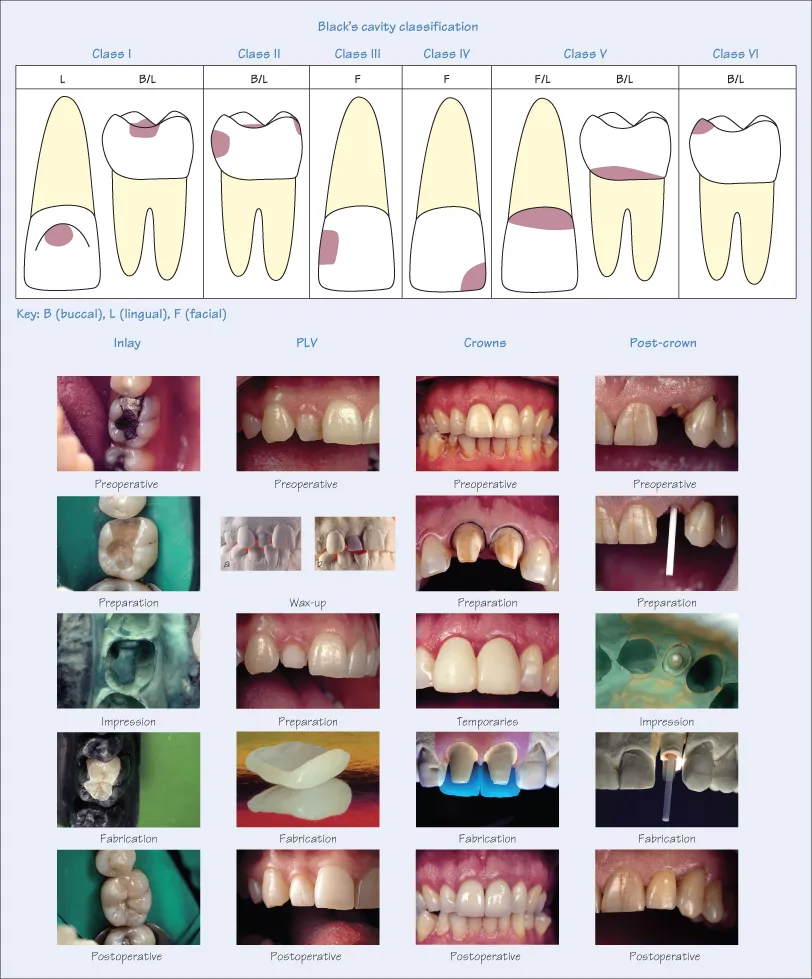
Intracoronal prostheses are defined as those surrounded by one or more natural tooth surface(s). This categorisation is broadly based on Black’s cavity classification:
- Class I: lesions of pits and fissures of all teeth, predominantly in premolars and molars;
- Class II: lesions on the proximal surfaces of posterior teeth, referred to as MO (mesial-occlusal), DO (disto-occlusal), and MOD (mesial-occlusal-distal);
- Class III: lesion in the anterior teeth, similar to a class II lesion, the class III lesion typically appears at the contact point;
- Class IV: the class IV lesion is a class III lesion including the incisal corner of an anterior tooth;
- Class V: typically occurs at the cervical margins on the buccal, rather than the lingual, aspect of any tooth;
- Class VI: not originally in Black’s classification, but has become accepted as an additional lesion that occurs on the tips and cusps of posterior teeth, or along the biting surfaces of the incisors.
Three developments have made Black’s cavity classification redundant. First, research has elucidated biological mechanisms such as demineralisation/remineralisation and the role of fluoride ion, and removal of infected and affected dentine is no longer a prerequisite. Second, new restorative materials such as resin (plastic)-based adhesives and filling materials, and therapeutic filling materials, which are both bacteriostatic and bactericidal, avoid removing vast amounts of tooth. Third, improved and sophisticated techniques such as adhesive protocols allow restorations of small lesions, preventing progression to larger cavities. All these advances preserve more of the natural tooth, and Black’s classification is therefore used today as a notation, rather than as a basis for restoring decay. Whereas, in the past, cavity design was geometric (dictated by the restorative material), it is now amorphous (dictated by the extent of disease).
Smaller lesions are restored by a direct approach, while larger Class II or Class IV are restored indirectly with inlays or onlays (extracoronal), when a direct approach is mechanically or aesthetically inferior. Inlays and onlays are fabricated in a dental laboratory using a variety of materials including composite resins, ceramics and cast gold alloys.
Indirect Extracoronal Prostheses
Extracoronal prostheses are defined as those surrounding one or more natural tooth surface(s). The indications for extracoronal restorations are:
- Restoring structurally compromised teeth;
- Improving function (e.g. altering occlusal vertical dimension – OVD);
- Improving aesthetics (e.g. anterior maxillary and mandibular sextant);
- Abutments for a fixed partial denture (FPD).
Extracoronal prostheses are categorised as:
- Inlays and onlays – the difference between an inlay and an onlay is the extent of tooth loss requiring replacement. Broadly speaking, an inlay ‘fits into’, while an onlay incorporates cuspal coverage and ‘fits onto’ the tooth;
- Porcelain laminate veneers (PLV) – the principal use of PLVs is improving anterior aesthetics by altering tooth morphology and colour. PLVs are the least invasive of extracoronal restorations, usually involving the buccal surfaces of anterior teeth. If the underlying tooth colour is acceptable, only minimal tooth reduction is necessary (0.3–0.8 mm) for improving shape and colour with a thin porcelain laminate fabricated in a dental laboratory. PLVs are the most prescribed type of restoration for purely cosmetic reasons. However, it should be remembered that preparing vital healthy teeth for PLVs with little aesthetic improvement is contentious, especially if similar results are achievable with less invasive protocols such as bleaching or composite resin fillings;
- Partial coverage crowns – partial coverage crowns are an extension of PLVs. They occupy a midpoint between full coverage and the minimally invasive PLV. Many configurations are possible, e.g. 1/2, 3/4, 7/8, etc. The rationale for partial coverage is retaining as much natural tooth substrate as possible, and hence preserving pulpal and structural integrity;
- Full coverage crowns and fixed partial dentures (FPD) or bridges – a full coverage, 360° crown is indicated for severely broken-down teeth, abutments for FPDs, or rarely for elective aesthetic treatment. Various materials are used for fabricating crowns depending on the clinical scenario, e.g. cast metal, metal-ceramic, all-ceramic, composite and acrylic. For vital teeth, a crown can be supported either by coronal dentine or a core build-up. For endodontically treated teeth a post-and-core complex may be necessary. Intraradicular posts are available in many materials, designs, configurations and sizes. A core can be fabricated directly in the mouth using amalgam or composite, or indirectly in a dental laboratory using cast metals or ceramics. The sole purpose of a post-and-core complex is supporting the eventual extracoronal crown. Posts and cores do not reinforce or strengthen teeth, but weaken an already compromised root and the remaining coronal dentine. A ferrule effect is highly desirable for cores (with or without posts);
- Combination prostheses – depending on the extent of the clinical requirements, any intra- and extracoronal restoration can be combined into a single entity, e.g. inlay + onlay or PLV + inlay (veneerlay).
Key Points
- A direct restoration is carried out chair-side, while an indirect restoration requires using a dental laboratory.
- Black’s classification, although redundant, is useful for describing the site of a lesion.
- Intracoronal restorations are surrounded by tooth surface(s).
- Extracoronal restorations surround tooth surface(s).
- Inlays are examples of intracoronal prostheses.
- Onlays, PLVs and crowns are examples of extracoronal prostheses.
2
Overview: Rehabilitation by Artificial Teeth
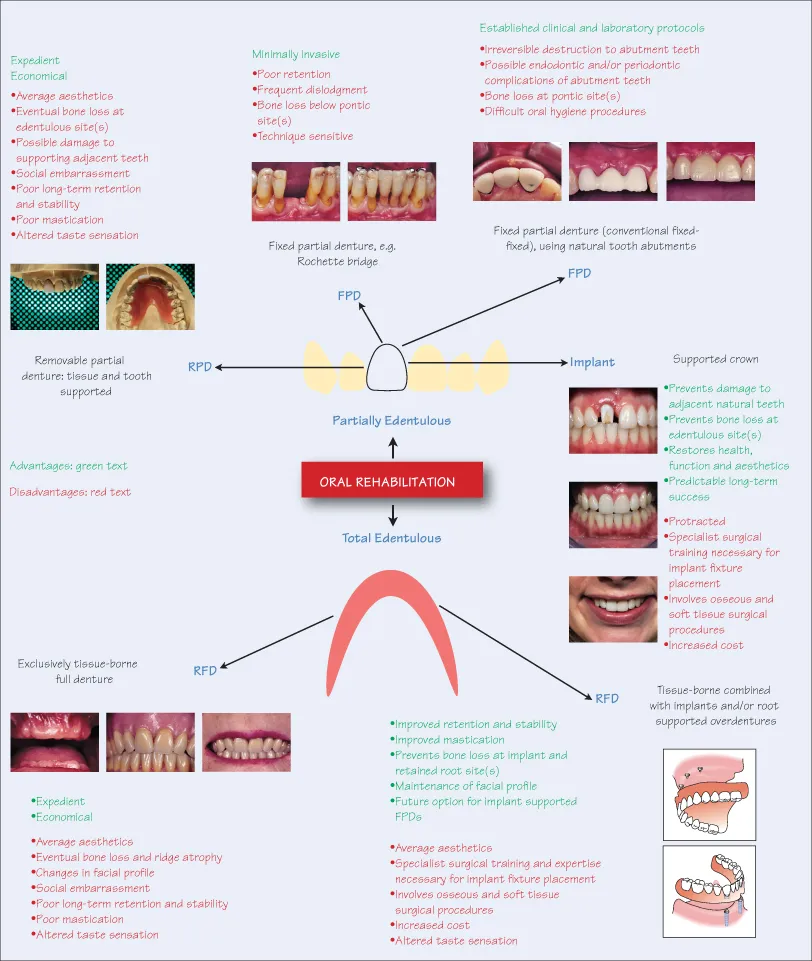
Oral rehabilitation of missing teeth is achieved with removable or fixed prostheses. The distinction between the two is that removable prostheses are supported by both soft tissues and teeth and/or implants, whereas fixed prostheses are exclusively supported by teeth and/or implants. Before deciding to replace missing teeth, the shortened arch concept should be considered.
Removable Full Dentures (RFD)
Edentulous rehabilitation is either with full/full dentures, totally supported by the alveolar ridges, or with overdentures supported by strategically placed implants and/or retained natural tooth roots for additional stability.
Removable Partial Dentures (RPD)
An RPD relies on support from both soft tissues and adjacent or surrounding natural teeth or implants. These dentures can be fabricated entirely from acrylic resins, or in combination with cast metal frameworks. Clasp, rests and precision attachments are often incorporated into the denture design for additional retention and stability. A variation of RPDs are overdentures, retained by tooth roots or mini implants.
Fixed Partial Dentures (FPD)
Before dental implants, fixed partial dentures were the state-of-the-art prostheses for replacing missing teeth, but involve gross tooth preparation of supporting abutments. More conservative FPDs, with minimal or no preparation, include Maryland, Rochette or fibre-reinforced bridges. While the advantages of minimal preparation are obvious, these types of bridge are less retentive, requiring frequent recementing and are often used as transitional protheses, e.g. during the surgical healing phase following bone grafting or implant placement. Other uses include splinting periodontally compromised mobile teeth, or as an interim restoration while awaiting a more permanent restoration.
Conventional FPDs require preparation of abutment teeth for supporting the final prosthesis incorporating pontic(s) for replacing missing tooth or teeth. Numerous FPD configurations are possible, e.g. fixed-fixed, cantilever, telescopic, with or without precision attachments for stress relief for long spans. FPDs have a cast metal substructure, which is subsequently veneered with porcelain. Newer all-ceramic FPDs use dense ceramic frameworks, e.g. of zirconia or alumina, for supporting the veneering porcelain. Although conventional FPDs using natural teeth as abutments are destructive, they still have a place in prosthodontics where local anatomy contraindicates surgery or implant placement. Besides natural tooth abutments, implants can also act as abutments for FPDs.
Dental Implants
Dental implants are titanium root forms placed into alveolar bone. Following osseointegration, the implants are prosthetically restored with a variety of artificial prostheses including RFD, RPD and FPD. Implants are extremely versat...
Table of contents
- Cover
- Titles in the dentistry At a Glance series
- Title page
- Copyright page
- Dedication
- Epigraph
- Preface
- Acknowledgements
- Section 1: Overview of prosthodontics
- Section 2: Diagnostics
- Section 3: Treatment planning
- Section 4: Occlusion
- Section 5: Periodontal aspects
- Section 6: Endodontic aspects
- Section 7: Anterior dental aesthetics
- Section 8: Intracoronal restorations
- Section 9: Extracoronal restorations
- Section 10: Materials for indirect restorations
- Section 11: Tooth preparation
- Section 12: Temporary restorations
- Section 13: Impressions
- Section 14: Dental laboratory
- Section 15: Cementation
- Section 16: Removable prostheses
- Section 17: Dental implants
- Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.4M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Prosthodontics at a Glance by Irfan Ahmad in PDF and/or ePUB format, as well as other popular books in Medicine & Dentistry. We have over one million books available in our catalogue for you to explore.