There is a no more rewarding experience in restorative dentistry than to duplicate to perfection the colour, texture and surface anatomy of the human tooth. Dental porcelain is the closest match to tooth enamel of all our restorative materials but is perhaps the most difficult to use in dental practice.A study of the science of dental porcelain will enable the dentist or technician to perfect his art since it develops an increasing awareness of the fundamental problems in construction.Preparation design, the stresses developing in porcelain restorations, the influence of opaque backgrounds on colour, surface reflectivity and light transmission in crowns are some of the complex factors that influence the success of a porcelain veneer restoration.A survey of metals, bonding systems, cements and impression materials will enable the clinician to select his materials with greater confidence. New research on the shoulder preparation for the veneer crown also sheds light on the controversy of the bevel versus the butt joint. The author has attempted to rationalise the use of both metal and alumina reinforced ceramics and to show how no ingle system can be applied universally if optimum aesthetics is to be achieved.
eBook - ePub
The Science and Art of Dental Ceramics - Volume I
The Nature of Dental Ceramics and their Clinical Use
- 331 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
The Science and Art of Dental Ceramics - Volume I
The Nature of Dental Ceramics and their Clinical Use
About this book
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
Monograph IV
Porcelain as a Restorative Material
What is the role of the porcelain veneer crown in restorative dentistry? To understand this problem it is essential, firstly, to consider the properties of porcelain in relation to resistance to plaque formation, ease of fabrication and maintenance of fit and occlusal stability. Only then can the clinician use this material to its best advantage. The excellent chemical resistance and stability of dental porcelain has already been described in Monograph I (The Nature of Dental Ceramics). This monograph is more concerned with the biological implications when using this material.
The role of dental plaque in causing periodontal disease and dental caries will probably be the most significant area of research in the next decade. This research will not only be confined to the hard and soft tissues in the mouth but also to the restorative materials used to replace these tissues. The susceptibility of various dental materials to accumulation of bacterial plaque is receiving increasing attention and a greater knowledge of these processes must enable the clinician to use his materials to better effect in combating dental disease.
The correct design of bridge pontics, the signifigance of tooth contour, surface integrity, and marginal seal of restorations in preserving the health of gingival tissue as well as tooth structure cannot be over-emphasized.
In addition, the study of occlusion and its greater understanding in the teaching schools will also offer the future graduate the opportunity of constructing restorations of a much higher standard than has been possible in the past.
Plaque Accumulation on Restorative Materials
Rough surfaces on any restorative material will increase the accumulation and retention of dental plaque (Swartz, and Phillips, 1957). It has also been shown that accumulation of dental plaque on tooth surfaces will produce an inflammatory response from gingival tissue (Loe et al., 1965). The degree of plaque formation on fixed restorations is therefore of paramount importance.
Glazed dental porcelain is the most easily cleansed material that is used in dentistry today. Although it has been shown that plaque can accumulate on dental porcelain in areas where it is not self-cleansing, these studies have perhaps confused the issue as to the material’s easy cleansability. Studies carried out on plaque formation occurring on the polished surfaces of pontics constructed of cast gold, acrylic resin and glazed porcelain showed no significant difference between any of the materials (Clayton and Green, 1970). It was also shown that all these materials may produce an inflammatory response in the residual ridge mucosa (Stein, 1966; Podshadley, 1968). There seems little doubt that there is no dental material available today that will actually resist plaque formation, and until such a material is produced it is of greater interest to the clinician to know what degrees of plaque accumulation are to be found on current restorative materials, where some cleansing action can be effective.

Fig. 4-1 12, 11 and 21, 22 prior to crowning. Gingival inflammation present particularly in the interdental papillae.

Fig. 4-2 12, 11 and 21, 22 after insertion of aluminous porcelain jacket crowns (Vitadur). Gingival condition shows a marked improvement after 5 years.
Newcomb (1974) found that plaque indices for porcelain were lower than those for homogeneous uncrowned teeth. The improvement in gingival condition of a patient’s teeth after crowning with aluminous porcelain jacket crowns is illustrated in Figs. 4-1 and 4-2 and supports Newcomb’s findings.
An earlier interesting study carried out by Kaqueler and Weiss (1970) on plaque accumulation on dental restorative materials revealed that in experiments performed, in vivo, on dogs, that significant differences did exist between various restorative materials. After periods of up to 19 days on a soft diet, the dogs’ teeth were painted with basic fuschine 1 percent and magnified colour pictures were taken. The staining reaction of the plaque showed consistently that plaque accumulation was greatest on the surface of unpolished amalgam, zinc phosphate cement, silicate cement, and finally glazed porcelain, which showed almost no accumulation except at the margin where it increased with time. This study confirms what many clinicians observe, that dental porcelain is the most self-cleansing of all our restorative materials. A simple example can often be seen where a single porcelain crown will appear lighter in shade than the surrounding teeth until these teeth are cleaned. By contrast an acrylic crown can often appear darker due to accumulation of plaque and surface stain.
However, in a recent study, Wise and Dykema (1975) showed that there was no statistical difference between the plaque-retaining capacities of freshly-polished acrylic resin and porcelain, but that porcelain had a statistically significant lower plaque-retaining capacity than for a ceramic high-fusing gold alloy. It is likely that the gingival inflammation often seen around acrylic resin crowns could be caused by rapid loss of polish due to wear, and also to marginal leakage, which is not improved by the low modulus of elasticity of acrylic resin and its high water absorption and thermal expansion.
Marginal Fit
A criticism levelled at the complete porcelain veneer crown (the porcelain jacket crown) is that it generally has “open margins”. By contrast the porcelain veneer metal-ceramic crown is often claimed to produce a better fit. However, it is possible by careful control of the porcelain build-up, to minimize the firing shrinkage and produce remarkably accurate fitting crowns. A technique for doing this has been described (McLean, 1970). Crowns made by this technique were cemented to jacket crown preparations in vivo using a polyether rubbera as the cementing medium (McLean, and von Fraunhofer, 1971). This rubber produced a film thickness of 22 µm when tested according to B.S. 3364 and simulated the performance of zinc phosphate or zinc polycarboxylate cements. The rubber film was removed from the crown and embedded in an epimine resin prior to sectioning and measuring the rubber’s thickness. A typical film thickness of rubber under one of the aluminous porcelain jacket crowns is illustrated in Fig. 4-3 and it may be seen that a maximum film thickness of 60 µm was recorded.
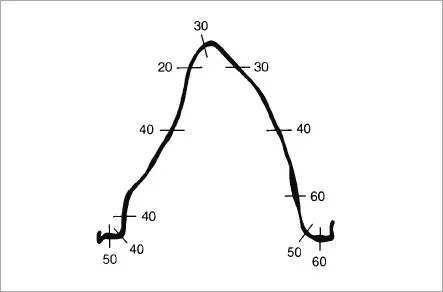
Fig. 4-3 Tracing of a typical Impregum “replica” of a cement film beneath an aluminous porcelain jacket crown in the labio-lingual plane, film thickness in microns. (After McLean, J. W., and von Fraunhofer, J. A. (1971) Brit. dent. J. 131:107.)
This study showed that a well-made aluminous porcelain jacket crown could be made to fit the tooth as well as a metal-ceramic crown, and that the space created by removal of the platinum foil shim may make a greater contribution to accuracy of seating than hitherto thought.
The clinician might be tempted to think that a gap under a metal-ceramic crown is less than is actually present, since fit is often assessed by probing at the wrong angle (Fig. 4-4). By contrast, any inaccuracy in the fit of a porcelain jacket crown made to a butt joint is much more easily detected (Fig. 4-5).
The merits of the bevel, deep chamfer and flat shoulder will be discussed later in this monograph, and the rationale behind them explained in scientific terms (see page 276).
Micro-leakage under Porcelain Crowns
Clinicians who have been in practice for long periods are often struck by the fact that seldom do they ever see secondary caries under a complete porcelain veneer crown. Many times these crowns can be quite an indifferent fit and yet the cement lute is intact. By contrast a gold crown can be of vastly superior fit and yet show signs of micro-leakage and secondary decay. What is the explanantion for this?
It is generally agreed that micro-leakage is caused by the following factors:
- Solubility of the cement under dental plaque.
- Changes in dimension of the restoration or cement due to thermal or occlusal stressing.
- Lack of adhesion between the tooth and cement or between the cement and crown material.
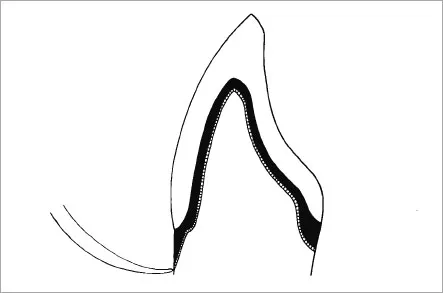
Fig. 4-4 Diagram showing incorrect angle ...
Table of contents
- Cover
- Title Page
- Copyright Page
- Foreword
- Preface
- Acknowledgements
- Table of Contents
- Introduction
- Monograph I – The Nature of Dental Ceramics
- Monograph II – The Strengthening of Dental Porcelain
- Monograph III – Aesthetics of Dental Porcelain
- Monograph IV – Porcelain as a Restorative Material
- Appendix
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access The Science and Art of Dental Ceramics - Volume I by John W. McLean in PDF and/or ePUB format, as well as other popular books in Medicine & Dentistry. We have over 1.5 million books available in our catalogue for you to explore.