Fear of pain is the number one reason people give for not making regular visits to the dentist. At the same time, a majority of dentists report experiencing anesthesia-related problems during restorative and endodontic dental procedures. If dentists are able to deliver painless treatment, patient compliance and satisfaction are likely to improve. Administration of local anesthesia is the first step of every dental procedure, and it affects the success of the entire appointment. If the patient is not adequately anesthetized, difficulties will arise. This book will help you successfully anesthetize your patients using the newest technology and drugs available. It presents the rationale, advantages, and limitations of the various anesthetic agents and routes of administration. Special emphasis is placed on supplemental anesthetic techniques that are essential to the practice of dentistry. This second edition brings the literature up to date and includes an expanded chapter on pulpal anesthesia.
eBook - ePub
Successful Local Anesthesia for Restorative Dentistry and Endodontics
Second Edition
- 240 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
Successful Local Anesthesia for Restorative Dentistry and Endodontics
Second Edition
About this book
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
| 1 | Clinical Factors Related to Local Anesthesia |
After reading this chapter, the practitioner should be able to:
• Discuss the clinical factors related to local anesthesia.
• Provide ways of confirming clinical anesthesia.
• Describe issues related to local anesthesia.
• Explain the effects anxiety has on local anesthesia.
• Discuss the use of vasoconstrictors.
• Characterize injection pain.
• Evaluate the use of topical anesthetics.
• Discuss alternative modes of reducing pain during injections.
Clinical pulpal anesthesia is dependent on the interaction of three major factors: (1) the dentist, (2) the patient, and (3) local anesthesia (Fig 1-1). The dentist is dependent on the local anesthesia agents as well as his or her technique. In addition, the dentist is dependent on the interaction with the patient (rapport/confidence). How the patient interacts with the administration of local anesthesia is determined by a number of clinical factors.
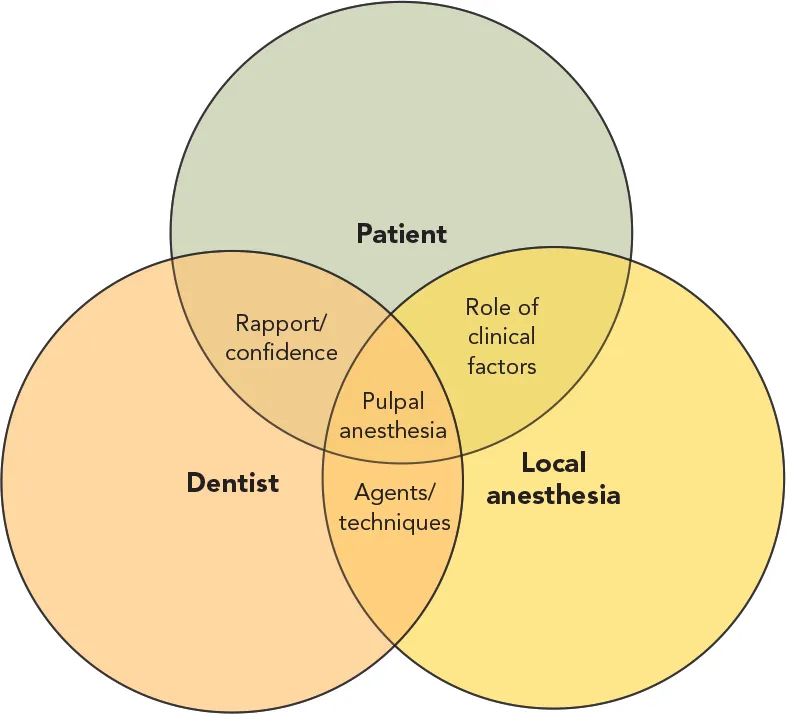
Fig 1-1 The relationship of pulpal anesthesia to the patient, dentist, and local anesthesia.
Confirming Pulpal Anesthesia in Nonpainful Vital Teeth
Lip numbness
A traditional method to confirm anesthesia usually involves questioning patients by asking if their lip is numb (Fig 1-2). Although lip numbness can be obtained 100% of the time, pulpal anesthesia may fail in the mandibular first molar in 23% of patients.1–16 Therefore, lip numbness does not always indicate pulpal anesthesia. However, lack of lip numbness for an inferior alveolar nerve block (IANB) does indicate that the injection was “missed,” and pulpal anesthesia will not be present.

Fig 1-2 Lip numbness does not guarantee pulpal anesthesia.
IN CONCLUSION, lip numbness does not always indicate pulpal anesthesia.
Soft tissue testing
Using a sharp explorer to “stick” the soft tissue (gingiva, mucosa, lip, tongue) in the area of nerve distribution (Fig 1-3) has a 90% to 100% incidence of success.2–5 Regardless, pulpal anesthesia may still not be present for the mandibular first molar in 23% of patients.1–16 Negative mucosal sticks usually indicate that the mucosal tissue is anesthetized.

Fig 1-3 A lack of patient response to mucosal or gingival “sticks” is a poor indicator of pulpal anesthesia.
IN CONCLUSION, the lack of patient response to sharp explorer sticks is a poor indicator of pulpal anesthesia.
Commencing with treatment
The problem with commencing treatment without confirming anesthesia is that there is no way to know if the patient is numb until we start to drill on the tooth. This may create anxiety for both the patient and the dentist. A typical scenario involving a crown preparation on a mandibular molar can become problematic if the patient feels pain when the mesiobuccal dentin is reached with the bur. If the patient reacts to the pain, the dentist may say, “Oh, did you feel that?” and then may try to continue with treatment. If the patient reacts again when the mesiobuccal dentin is touched with the bur, the dentist may try to work around the pain the patient is feeling by saying, “I’ll be done in a minute.” Such a situation would not make a good day for the dentist or the patient.
IN CONCLUSION, commencing with treatment without confirming anesthesia may add apprehension for the dentist and patient because neither one knows if the tooth is anesthetized.
Cold refrigerant or electric pulp testing
A more objective measurement of anesthesia in nonpainful vital teeth is obtained with an application of a cold refrigerant of 1,1,1,2-tetrafluoroethane or by using an electric pulp tester (EPT). Cold refrigerant or the EPT can be used to test the tooth under treatment for pulpal anesthesia prior to beginning a clinical procedure.17–20 A dental assistant could test the tooth to determine when pulpal anesthesia is obtained and then inform the dentist that treatment can be started.
In a very anxious patient, the use of pulp testing may cause a very painful reaction. Apprehensive patients can become sufficiently keyed up to react to even minimal stimulation. They may say, “Of course I jumped, it hurts!” or “It’s only normal to jump when you know it is going to hurt.”
IN CONCLUSION, pulp testing with a cold refrigerant or an EPT will indicate if the patient has pulpal anesthesia. For anxious patients, pulp testing may need to be postponed until the patient can be conditioned to accept noninvasive diagnostic procedures.
Cold testing
A cold refrigerant tetrafluoroethylene (Hygenic Endo-Ice, Coltène/Whaledent) (Fig 1-4) can be used to test for pulpal anesthesia before commencing drilling on the tooth. The technique for cold testing is quick and easy; it takes only seconds to complete and does not require special equipment. Once the patient is experiencing profound lip numbness, the cold refrigerant is sprayed on a large cotton pellet held with cotton tweezers21 (Fig 1-5). The cold pellet is then placed on the tooth (Fig 1-6). If clinical anesthesia has been successful, applications of cold refrigerant should not be felt. If the patient feels pain with application of the cold, supplemental injections should be given. If no pain is felt with the cold, it is likely that pulpal anesthesia has been obtained. Testing with a cold refrigerant is more convenient than with an EPT and gives a good indication of clinical anesthesia.
Fig 1-4 A cold refrigerant may be used to test for pulpal anesthesia before the start of a clinical procedure. (Courtesy of Coltène/Whaledent.)

Fig 1-5 The cold refrigerant is sprayed on a large cotton pellet.

Fig 1-6 The pellet with the cold refrigerant is applied to the surface of the tooth.
Pulp testing with a cold refrigerant can be performed effectively on gold crowns and porcelain-fused-to-metal crowns. In fact, pulp testing is fairly easy to use in these situations because the metal conducts the cold very nicely. Miller and coauthors21 also showed that pulp testing with a cold refrigerant is effective for all-ceramic crowns.
IN CONCLUSION, pulp testing with a cold refrigerant is a reliable way to confirm clinical pulpal anesthesia, even in teeth with gold, porcelain-fused-to-metal, and all-ceramic crowns.
Electric pulp testing
In order to use the EPT (Kerr Vitality Scanner, SybronEndo) (Fig 1-7), the tooth should be dried with a gauze pad or cotton roll. Toothpaste is applied to the probe tip of the pulp tester before placing the tip on the middle of the labial surface (for anterior teeth) or buccal surface (for posterior teeth) of the tooth to be anesthetized (Fig 1-8). The Kerr EPT automatically starts on contact with t...
Table of contents
- Cover
- Half Title Page
- Title Page
- Copyright Page
- Contents
- Preface
- Acknowledgments
- 1 Clinical Factors Related to Local Anesthesia
- 2 Mandibular Anesthesia
- 3 Maxillary Anesthesia
- 4 Supplemental Anesthesia
- 5 Clinical Tips for Management of Routine Restorative Procedures
- 6 Endodontic Anesthesia
- 7 Clinical Tips for Management of Specific Endodontic Situations
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Successful Local Anesthesia for Restorative Dentistry and Endodontics by Al Reader,John Nusstein,Melissa Drum in PDF and/or ePUB format, as well as other popular books in Medicine & Dentistry. We have over 1.5 million books available in our catalogue for you to explore.