This textbook provides an overview of the RPD design philosophy developed by Prof F. J. Kratochvil. His "RPI system"—a clasp assembly consisting of a rest, a proximal plate, and an I-bar retainer—changed how clinicians approach partial denture design. Topics in this book include RPD components and functions, design sequences for maxillary and mandibular RPDs, and techniques for surveying and determining the most advantageous treatment position. The authors provide illustrations of clinical cases throughout the book as well as an illustrated glossary of prosthodontic terminology. This book will prepare students and general practitioners to design and fabricate a biomechanically sound RPD framework for just about any dental configuration they encounter.
eBook - ePub
Kratochvil's Fundamentals of Removable Partial Dentures
- 240 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
Kratochvil's Fundamentals of Removable Partial Dentures
About this book
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information

Professor F. J. Kratochvil was one of the first to recognize the importance of biomechanics in the design of removable partial dentures (RPDs) and used these principles to develop a whole new design philosophy. It is the purpose of this book to present this philosophy. His initial publication1 forever changed the way in which dentists approached RPD design. Although he is most often associated with the use of the I-bar retainer, the reader should understand that he stressed the totality of RPD design and recognized the important role of other major components in the successful use of the I-bar retainer. Obviously, the I-bar retainer was an important component of his design philosophy, but the design of the guide planes and proximal plates were also fundamental. Because the I-bar has a relatively low retentive value compared to other retainer designs, its effectiveness is dependent upon the horizontal stability provided by the minor connectors and the proximal plates, and these portions of the RPD are integral to his design philosophy. He believed that there was no such thing as a simple I-bar RPD, just as there is no one technique that serves as a panacea for all clinical situations.
RPDs will continue to be one of the primary methods used to restore the missing dentition of partially edentulous patients in the foreseeable future, and consequently, it will continue to be important for dentists to be intimately familiar with the basic principles of RPD design and fabrication. The recent innovation in digital technologies will change the manner in which we design and fabricate RPDs, but the laws of biomechanics, and therefore the principles of RPD design that Kratochvil established, will not change.
Treatment of partially edentulous patients with RPDs has become increasingly sophisticated in recent decades, and when this treatment is planned and executed properly it will help to preserve the existing structures. In contrast, a poorly designed and fabricated RPD can trigger resorption of bony bearing surfaces and accelerate the loss of remaining dentition. Unfortunately, in recent years, curriculum time devoted to RPDs has been significantly reduced in many dental schools, and those directing the curriculum often lack appropriate training, experience, and educational resources. The result of this change has been startling. In recent surveys of dental laboratories in the United States, more than 90% of casts submitted lacked visible rests and RPD designs. Many students graduate from dental school without fabricating an RPD for a patient. In many studies, significant numbers of RPDs do not meet even half of the usual and customary design standards.2
The widespread perception that the health of the remaining teeth is compromised by RPDs as compared to other forms of treatment is not supported by the evidence. Studies comparing the outcomes of fixed dental prostheses (FDPs) and RPDs have indicated no differences in periodontal health of abutment teeth between the groups. The only differences noted in these studies were the higher levels of maintenance required by RPDs.3,4
The number of partially edentulous patients continues to increase as the population in most developed countries continues to age. Often times the only viable treatment option available to most patients is to restore the integrity of the dental arch and replace the missing dentition with an RPD. There are several reasons for this. In many patients, FDPs are not indicated, such as when the edentulous span is too great or in edentulous extension areas. Also, cost precludes the use of dental implants in most patients.
RPDs Versus Implants
It is quite clear that the expanding need for tooth replacement cannot be met with osseointegrated implants. In the United States, the number of partially edentulous patients restored with dental implants is expected to plateau at 3% to 5% of those potentially in need of this service. Cost is an important factor, but there are several other reasons for this phenomenon. An interesting paper published several years ago by Bassi et al5 illustrates the impact of additional factors. Forty consecutive partially edentulous patients seeking implant therapy were screened at the dental clinic at the University of Turin. Only 1 out of the 40 patients was ultimately restored with osseointegrated implants. There were a variety of reasons why implant therapy was not delivered to the other 39 patients. Many patients were not suitable candidates because they lacked sufficient bone volume at the desired sites. Another group, upon questioning, were happy with their RPDs, while another, when described the nature of the surgery to place the implants and/or enhance the potential implant sites, declined to undergo the surgery.
Another factor to consider is that the functional outcomes achieved with RPDs are comparable to those achieved with implant-supported FDPs. In the late 1980s and early 1990s, Kapur et al3,6-9 conducted a randomized clinical trial comparing the mastication efficiency of implant-supported FDPs with extension base (tooth-mucosal borne) RPDs (Fig 1-1). Both treatments were equally effective in improving chewing function. A large number of patients in both groups expressed satisfaction with their prostheses, but as expected, the level of patient satisfaction was higher in the fixed implant-supported group. Similar outcomes were recently reported by Nogawa et al.10 Kapur et al3,6-9 concluded that despite the superiority of the implant-supported FDPs in terms of patient satisfaction, lack of functional differences and success rates do not support the selection of implant-supported FDPs over RPDs, without consideration of other factors.

Fig 1-1 (a) Bilateral extension-base RPD. (Courtesy of Dr R. Faulkner, Cincinnati, Ohio.) (b) Bilateral extension areas restored with a single implant connected to a natural tooth abutment. The mastication efficiency of the RPD is equivalent to that obtained with the implant- supported FDP.
Moreover, implants cannot be used in many patients in need of tooth replacement in the posterior quadrants because of pneumatization of the maxillary sinuses or insufficient bone over the inferior alveolar nerve in the mandible (Fig 1-2). Sinus augmentation has become common in recent years, and the success rates of implants placed into these sites is quite good. However, the high cost of this procedure plus the cost of implant placement precludes most patients from selecting this option. In the mandible, most patients missing dentition in the posterior quadrant lack sufficient bone volume over the inferior alveolar nerve for implant placement, and the development of predictable procedures aimed at supplementing the vertical height of these bony sites has proved illusive.

Fig 1-2 (a) Pneumatized maxillary sinus. (b) Resorption of bone over the inferior alveolar nerve. Both preclude implant placement in the absence of site enhancement.
Short, wide-diameter implants in these sites have not obtained an acceptable level of success.11,12 The reasons for this are now becoming clear and include not only the length of the implants but also the lack of width of the alveolar bone to enclose the implant (Fig 1-3). Lateralizing the inferior alveolar nerve enables the placement of implants of suitable length. However, the morbidity associated with injury to the nerve can be quite significant.13

Fig 1-3 (a) Implant-supported FDP at delivery. (b) Bone levels 2 years after delivery. (c) Bone levels 5 years after delivery.
A typical partially edentulous patient is shown in Fig 1-4. The patient is missing posterior dentition in both the maxilla and mandible. Numerous spaces and diastemata have developed, destroying the integrity of both arches. Multiple teeth exhibit erosion and wear. Occlusal vertical dimension has been lost, reducing the height of the face and compromising facial esthetics. With proper treatment this dentition can be saved, the integrity of the arch restored, missing teeth replaced, and occlusal function restored to reasonable levels. Restoring the occlusal vertical dimension will dramatically improve facial esthetics. The purpose of this text is to delineate a treatment approach and RPD design principles that will consistently lead to favorable long-term treatment outcomes in such patients.
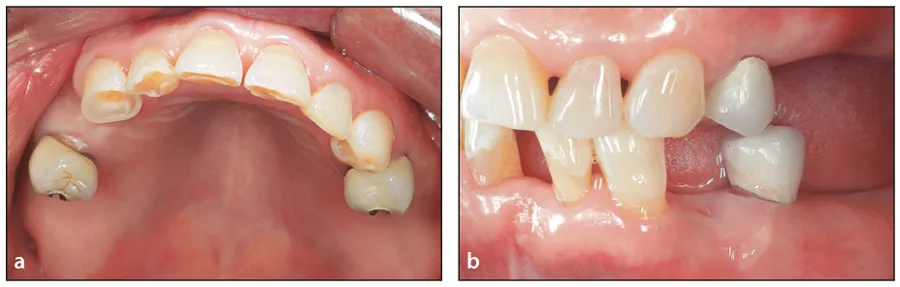
Fig 1-4 (a and b) Typical partially edentulous patient with multiple missing posterior teeth, lost occlusal vertical dimension, and loss of arch integrity. (Courtesy of Dr A. Davodi, Beverly Hills, California.)
Objectives of Treatment: The Partially Edentulous Patient
When teeth are lost, the remaining dentition loses the interproximal contacts that permitted the intact arch to function as a continuous unit. Loss of integrity is one of the first steps toward disorg...
Table of contents
- Cover
- Half Title
- Title Page
- Copyright Page
- Dedication
- Contents
- Preface
- Contributors
- 1 Introduction to Removable Partial Dentures
- 2 Removable Denture Rests
- 3 The Tooth-Tissue Junction and Proximal Plate Design
- 4 Major Connectors, Minor Connectors, and Denture Base Connectors
- 5 Retainers, Clasp Assemblies, and Indirect Retainers
- 6 Types of RPDs, Biomechanics, and Design Principles
- 7 Partial Denture Design Principles and Design Sequence
- 8 Surveying and Determining the Most Advantageous Treatment Position
- 9 Diagnosis, Treatment Planning, and Intraoral Preparation
- 10 Impressions for the RPD Framework and Laboratory Instructions
- 11 RPD Digital Design and Manufacturing
- 12 Physiologic Adjustment of the RPD Casting and Altered Cast Impressions
- 13 Maxillomandibular Records and Occlusion for RPDs
- 14 Optimizing Esthetics: Attachments and Rotational Path RPDs
- 15 Surveyed Crowns and Combined Fixed RPD Cases
- 16 Overlay RPDs Using Retained Roots and Implants
- 17 Using the RPI System for Defects of the Maxilla and Mandible
- 18 Treatment Removable Partial Dentures
- 19 Insertion and Maintenance of RPDs
- 20 Clinical Appointment Sequence
- Glossary
- Index
- Back Cover
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Kratochvil's Fundamentals of Removable Partial Dentures by Ting-Ling Chang,Daniela Orellana,John Beumer III in PDF and/or ePUB format, as well as other popular books in Medicine & Dentistry. We have over 1.5 million books available in our catalogue for you to explore.