![]()
1
Radiographic technique
Regardless of the reason for undertaking any radiographic study, the primary objective is to obtain high-quality diagnostic images, while ensuring the safety of the patient and personnel. This can be accomplished through preparation before the procedure and proper radiographic technique: using suitable radiographic equipment (X-ray generation and image formation), patient preparation and restraint, positioning and positioning aids, radiation safety equipment and protective barriers, and post-image capture quality assurance and processing.
The principles of X-ray generation and image production for wildlife species are no different than those for domestic species and are not discussed in detail here. There are several excellent radiology texts that provide this information (Capello and Lennox 2008; Silverman and Tell 2010; Thrall 2013). There are, however, some special considerations inherent in radiographing wildlife species. These primarily relate to the need for safe and humane restraint, and to radiographing small species, which are frequently encountered in zoo and wildlife practice.
There are several fundamental tenets of radiographic technique that are worth reinforcing.
• Take two views at 90° (orthogonal views) whenever possible. This is useful for thorough evaluation of both soft tissue and skeletal anatomy and pathology.
• One joint should be included in every long bone image. As long bone joints are usually characteristic, they assist with identification of the bone adjacent to the joint. In addition, the joint provides a reference point, allows consistency in serial imaging, may guide surgical decisions when located near pathology and may assist in assessing the maturity of the patient through the degree of physeal closure.
• The comparative view. This is mainly relevant to the appendicular skeleton, where imaging the contralateral side may be useful when the clinician is unfamiliar with normal anatomy or a comparison view may assist in confirming a diagnosis.
• Image labelling. All images must be labelled with patient information (at a minimum, the species and individual animal identifier such as a transponder, band, tag or accession number) and side markers (left or right). Labels indicating the view may be useful.
• Review previous images. This will allow the clinician to more adequately plan a radiographic study, become familiar with previous or pre-existing pathology and review radiographic anatomy.
• Peer or specialist review of images. This is particularly valuable if the clinician is less familiar with a species, or with the subtle radiographic changes that may be associated with particular disease processes (e.g. pulmonary disease). It will result in improved patient care and assist in the development of radiographic technique and interpretation skills, which is particularly valuable for wildlife because information on many species and disease processes is limited. The review process is now relatively straightforward with PACS (picture archiving and communication systems) whereby digital images can be readily transferred using various web-based platforms. The universal image format for PACS is DICOM (digital imaging and communications in medicine). Digital images can also be saved in different formats (jpeg, tiff) and sent via e-mail.
Digital radiography
Digital radiography has revolutionised radiology because of improved image quality; superior image contrast; greater exposure latitude; immediate viewing; reduced need for repeat exposures caused by incorrect exposure factors and film processing errors; the ability to manipulate images; the ability to electronically transmit data to an appropriate storage medium from which it can be electronically retrieved; reduced physical storage space of images; and ease of electronically transferring images.
However, despite these advantages over conventional screen-film (SF) systems, getting the most out of a digital system requires an understanding of the principles of digital imaging. SF technique is not necessarily applicable to digital radiography and may be counter-intuitive. A common misconception is that digital systems correct for exposure errors, when in fact they do not. During the analysis of the image data, the potential exists for the digital system to make adjustments to the image data so that the image has an acceptable level of brightness in the presence of underexposure and overexposure. However, the exposure error remains regardless of what occurs during image processing by the system’s software (Herrmann et al. 2012).
Two digital radiographic systems are currently available: computed radiography (CR) and direct digital radiography (DR). The primary difference between the two systems is the method by which the X-ray photons are captured and converted to a digital image. The component of these systems where this occurs is in the digital receptor (digital detector, flat-panel detector, sensor plate), which is the plate that receives the X-ray photons after they pass through the patient. In the case of CR, it is a flexible plate coated with a photostimulable phosphor (PSP) that temporarily stores a latent image of the X-ray attenuation pattern of the patient. The latent image is read optically as photostimulated luminescence when the PSP plate is subsequently stimulated using a scanning laser. The CR cassette must be processed in a plate reader following exposure (Robertson and Thrall 2013). In the case of DR, the transmitted X-ray signal is read immediately after exposure and converted to an electronic file within the receptor plate and therefore does not use a cassette (Williams et al. 2007; Robertson and Thrall 2013).
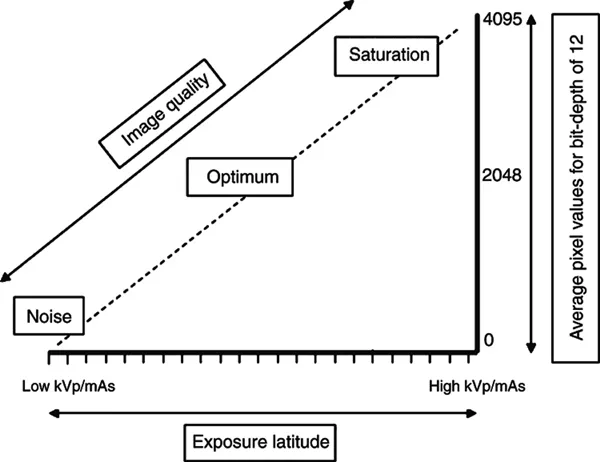
After the X-ray photons pass through the patient, digital receptors sense their intensity variation over an area, from which a matrix of many individual picture elements or pixels is formed. Each pixel is represented by an intensity value that equates to a shade of grey. This value ranges from black (0) to white (2x – 1), where x is the bit-depth and equates to the number of possible grey shades in a pixel. A greater bit-depth means a higher number of independent shades of grey that can be represented by each pixel. For example, these intensity values will be 0–255 (28), 0–1023 (210) or 0–4095 (212) for bit-depths of 8, 10 and 12, respectively. The number of available grey shades for each pixel will influence the contrast of the image. If a pixel has only a few grey shades, the image can only have a very narrow range of contrast because there will be only black pixels, white pixels and pixels of a few grey shades. If, conversely, there are many grey shade options for each pixel, the scale of contrast can be long. A typical digital receptor has a linear relationship between exposure and the resulting pixel value (Fig. 1.1). Low exposures result in low pixel values and higher exposures give greater pixel values. The usefulness of bit-depth becomes apparent in the image post processing. A high bit-depth provides much greater latitude for adjusting image contrast and brightness. A low bit-depth results in very limited range of adjustment, where the difference between dark and bright in the grey scale is narrow. Achieving the optimal image therefore requires the selection of appropriate exposure factors for a particular body part or patient size, as well as familiarity with the capability of the system being used (Robertson and Thrall 2013; Sprawls 2014).
Figure 1.1: Relationship between exposure, average pixel values and image quality.
The number of pixels per inch or centimetre (PPI, PPCM) is a measurement of the pixel density in a system and determines the spatial resolution. This relates to the ability of an imaging system to allow two adjacent structures to be visualised as separate (the distinctness or sharpness of an edge in the image). The greater the PPI/PPCM, the greater the spatial resolution, which in turn gives the impression of greater detail. Other factors contributing to spatial resolution are X-ray tube focal spot size, collimation, scatter, grid efficiency and motion of the patient.
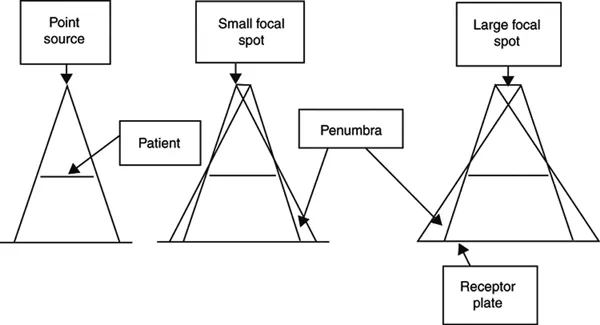
The focal spot of the X-ray machine is the area on the anode of the X-ray tube struck by electrons from which the resulting X-ray photons are emitted. The smaller the focal spot the sharper the image. A large focal spot reduces image quality by reducing the ability to define small structures, and the edges of anatomical structures are less sharp, which is called ‘penumbra’ (Fig. 1.2) (Robertson and Thrall 2013). The focal spot size cannot be altered; however, some X-ray machines provide two filaments of different sizes to make a dual-focus tube, adding flexibility to the system.
Figure 1.2: Diagram illustrating the effect of focal spot size on image quality. Large focal spot size results in loss of detail, whereas a small focal spot produces sharper images. Adapted from Radiology, 16, Gorham and Brennan, Impact of focal spot size on radiologic image quality: A visual grading analysis, 304–313, Copyright 2010, with permission from Elsevier.
Collimation of the beam to the appropriate region of interest is equally as important with digital radiography as it is with SF radiography. Limiting the area that receives radiation reduces the patient’s dose and minimises scatter radiation to the digital receptor. Digital receptors are more sensitive to low levels of radiation and the resulting digital image might have reduced contrast because of excess scatter radiation striking the receptor. Close collimation will improve contrast and wide collimation may result in more grey and less detail. However, care must be taken with close collimation to ensure annotation of the image does not obscure the structures of interest. Some digital receptors also require a minimum area of the receptor to be exposed to enable effective image formation. Post-processing cropping should not be used as a replacement for beam restriction achieved through physical collimation before capturing the image (Herrmann et al. 2012). The primary beam must be centred on the centre of the digital receptor.
Although antiscatter grids can be used in digital radiography, some manufacturers have incorporated a scatter-correction algorithm into the image-processing software, which makes grid use unnecessary. Antiscatter grids may be recommended for large patients. If an antiscatter grid is to be used, it must be specific for the digital receptor being used (Robertson and Thrall 2013).
Patient motion because of poor patient restraint or long exposure time (s) may result in blurred images. Short exposure times minimise motion artefact associated with rapid respiratory rates or muscular tremors (Silverman and Tell 2010).
A characteristic of digital systems is the ability to correct for exposure deficiencies to a much greater degree than with SF systems and thus create an image of suitable quality that is relatively independent of the kVp and mAs values selected. This is because of the greater dynamic range of digital receptors and the software capabilities of digital systems. The dynamic range of a digital receptor is the ratio between the maximum and minimum X-ray intensities that can be detected. For all systems, the smallest useful intensity is determined by the intrinsic system noise. The largest intensity is determined by receptor saturation (Williams et al. 2007). For example, if the minimum exposure that the receptor can detect is low and the ...