Rehabilitation of cerebral visual disorders in the framework of visual neuroscience
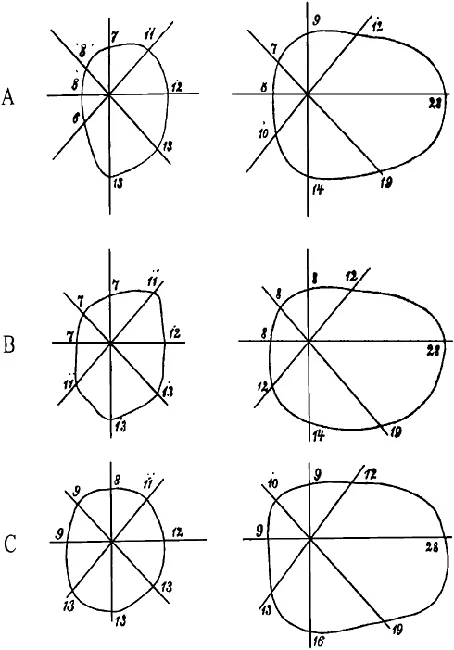
From the very beginning of neuroscience, vision research has mainly been concerned with the elucidation of the nature of various visual deficits and the identification of the location of brain injury responsible for these deficits (Zeki, 1993). Early clinical reports on patients showing selective loss of visual functions and abilities following acquired posterior brain injury have suggested a functional segregation of the visual cortex, a concept that many years later has been verified on the basis of combined anatomical, electrophysiological and behavioural evidence (Desimone & Ungerleider, 1989; Grill-Spector & Malach, 2004; Zeki, 1993). Enormous progress has been made in understanding the neurobiological basis of visual perception and the neuropsychology of vision is still a major topic in neuroscience. However, this progress is not reflected in the study of recovery of visual function in patients with acquired brain injury. The related findings are not included in neuropsychological rehabilitation, possibly because visual-perceptual disorders are not considered as cognitive deficits (see, for example, Cicerone et al., 2005; Halligan & Wade, 2005; Ponsford, 2004). At first sight, this is difficult to understand given the fact that about 30% of patients with acquired brain injury suffer from visual disorders (Clarke, 2005; Hier, Mondlock & Caplan, 1983a; Rowe et al., 2009; Sarno & Sarno, 1979; Suchoff et al., 2008). Furthermore, visual disorders often either directly affect cognitive performance or exacerbate cognitive deficits (Uzzell, Dolinskas, & Langfitt, 1988), which may interfere with the rehabilitation of other cognitive impairments and impede vocational rehabilitation efforts (Groswasser, Cohen & Blankstein, 1990; Patel, Duncan, Lai, & Studenski, 2000; Reding & Potes, 1988; Rowe et al., 2009). However, it does not seem that a lack of interest in the recovery of vision or visual rehabilitation can account for the fact that the advances in understanding the neurobiological basis of visual perception have not led to greater progress in neuropsychological rehabilitation. As early as 1867, Zagorski reported the case of a 35-year-old lady who complained of loss of vision on the left side. Perimetric testing revealed a complete left-sided hemianopia, probably caused by a right-sided occipital haemorrhage. Eight days later the patient noticed return of light vision in her left hemifield; 6 weeks later she reported having full vision again. Weekly visual field measurements were in agreement with the patient’s reports: the region of blindness shrank successively and vision eventually returned to the left hemifield (see Figure 1.1). Zagorski’s single case report is probably the first report on recovery of vision after acquired brain injury. In their “Handbook for Neurologists and Ophthalmologists” [author’s translation] Wilbrand and Saenger (1917) dedicated a comprehensive chapter to the natural course of complete cerebral blindness. According to their observations, vision recovered first in one hemifield; a few cases later showed complete return of vision in both hemifields. In most cases recovery of vision took place within hours or days; in some patients, however, the process of recovery was much slower and was not completed for several weeks. A similar course was observed in subjects with homonymous hemianopia. In the same year (1917/1990), Poppelreuter published his monograph on visual disturbances after occipital gunshot wounds, in which he reported not only the results of his detailed diagnostic visual disorders assessment, but also his observations on spontaneous recovery and the effect of systematic treatment. Poppelreuter preferred an experimental approach for assessing and treating his patients. In his view, conventional assessment and treatment methods were too “crude” (i.e., inaccurate), and systematic rehabilitation measures did not exist. His approach was also very pragmatic, i.e., ecologically valid, which is exemplified by his statement that “any intervention should, at the very least, have as its aim that the man should again be able to converse comprehensibly, to write his own letters, to read a newspaper, and to calculate his expenses by himself” (p. 5). Poppelreuter pointed out that functional impairment in vision in the acute stage may often be exaggerated since unspecific cognitive and affective alterations can affect the use of spared visual capacities. Since complete spontaneous recovery was the exception rather than the rule in his patients, rehabilitation measures were required to reduce their visual handicap and improve their independency in daily life activities and, thus, their “usefulness for society”. Poppelreuter was aware of the difficulty of attributing an improvement unequivocally to the treatment: “Only exact control of the effect [of treatment] offers a substantial argument for the systematic training effect over a short period of time, namely using a work task which remains constant” (p. 240). He developed training methods that specifically aimed at improving the reading impairments in patients with visual field loss (i.e., hemianopic dyslexia), which have already been described by Mauthner in 1881 and Wilbrand in 1907 (see Schuett, Heywood, Kentridge & Zihl, 2008a, for a comprehensive review). Poppelreuter correctly noticed that parafoveal field loss is not only associated with impaired global text processing but also with an impairment of the “co-ordination of the reading gaze-shifts”, which becomes manifest as a distortion of the typical, staircase-like oculomotor reading pattern. He therefore taught patients to compensate for
their field loss by systematically shifting their fixation from the beginning to the end of a line. The resulting improvement in reading performance is the first known example for the substitution of visual field loss by oculomotor activities. According to Poppelreuter, the substitution of an impaired function (the parafoveal visual field) by another, intact function (eye movements) critically depends on whether the replacement function also contributes to the visual capacity or performance in question under normal circumstance.
Yet, Poppelreuter’s observations on the recovery of vision after brain injury and his experiences with the systematic treatment of visually disabled, brain-injured patients as well as on the recovery of visual function in patients with occipital injury have largely been neglected in the literature. Even in the classic monograph by Teuber, Battersby, and Bender (1960) on visual disturbances, only few qualitative data are reported on the recovery of visual functions in a similar group of cases (Second World War soldiers) with missile wounds to the brain. Teuber (1975) reported follow-up observations in 520 soldiers with occipital gunshot injuries and confirmed Poppelreuter’s observation that vision can reappear in affected visual field regions.
In contrast to the diminishing interest in the study of recovery of vision after brain injury in humans after the end of the First World War, there was a growing interest among brain researchers in studying the effects of experimentally induced lesions to brain structures subserving vision in animals. It was Klüver (1942), especially, who studied the effect of experimentally induced brain lesions on vision in monkeys and found that bilateral occipital injury results in a profound but not total loss of visual information processing capacity. Yet, it required a “sufficiently long period of training” before the monkey was able to, for example, locate objects in space. A famous single case study on a rhesus monkey, Helen, from whom the striate cortex was almost totally removed bilaterally, and who was studied intensively over a period of 8 years (Humphrey, 1974), revealed that the monkey could regain an effective, though limited, degree of visually guided behaviour by practice in natural environments. Cowey (1967) and Weiskrantz and Cowey (1970) convincingly showed that practice can reduce the size of a cortical, but not a retinal, scotoma in monkeys, as defined by the animal’s ability to detect light targets. An even more complete and specific recovery of vision was demonstrated by Mohler and Wurtz (1977). Deficits in the detection of light stimuli in the affected field region as well as in saccadic localisation accuracy disappeared 6 weeks after the lesions had been induced. Again, systematic practice was necessary for recovery, which was mainly observed in the portion of the scotoma that had been subjected to practice. Thus, injury to the striate cortex does not always result in an irreversible, absolute loss of vision, but systematic treatment is required for its return. However, the results obtained in animal studies cannot directly be transferred to patients. It has, for example, been shown that patients can also accurately respond to light stimuli presented in their cortical scotoma. This phenomenon has been coined “blindsight”, since patients are never aware of the presence of the target. Demonstrating this phenomenon requires special testing conditions and typically patients do not show it without systematic practice of the task (see Danckert & Rosetti, 2005; Weiskrantz, 2004, for comprehensive reviews). It is still an open issue whether this “residual visual capacity” is due to recovery, residual functioning of spared visual cortex, or represents a visual function that is based on extrageniculo-striate mechanisms that were not affected by injury. However, “blindsight” does not seem to reduce patients’ visual disability because they cannot make use of this sub- or unconscious visual function (Zihl, 1980). Thus, although there is no doubt that in human subjects showing this capacity visual processing takes place in the “cortically blind”field region (like in monkeys with cortical scotoma), nobody would go so far as to consider a patient showing blindsight “visually rehabilitated”. Nevertheless, visual brain lesion research in primates has contributed substantially to our understanding of the recovery of visual function in humans. On the one hand, monkeys show considerable return of both elementary and complex visual function after intensive and systematic training to overcome the deficit. On the other hand, these experiments demonstrate that total and irreversible loss of a particular visual capacity is only to be expected if more than one structure of the neural network subserving this capacity is injured (see, for example, Frommer, 1978; Rothi & Horner, 1983; Stein, 1994, for reviews). As already shown by Mohler and Wurtz (1977), monkeys no longer recover from blindness after striate cortex injury when their ipsilateral colliculus superior has also been destroyed. Thus, both the site and the size of the lesion appear critical in the study of recovery of vision and adaptation to visual field loss after brain injury.
Recovery of function: Restitution vs. substitution
The first and foremost question in rehabilitation after brain injury is whether there is any recovery potential at all. If a particular visual function depends entirely on one single cortical structure, and if this structure is completely and irreversibly injured, then recovery of the affected visual function cannot be expected. Unfortunately, and despite enormous improvements in brain imaging techniques (Johansen-Berg, 2007), the definition of reversibility and irreversibility of brain injury is still an open issue. In cases of spontaneous recovery it is, of course, reasonable to assume that brain injury merely had reversible consequences (see Bosley et al., 1987). But does the opposite also always hold true, namely that the brain structure in question has really undergone irreversible injury when no spontaneous recovery occurs? Another important but similarly difficult question concerns the cortical representation of visual functions. “Functional specialisation” does not imply strict localisation of function. If it did, then injury to a particular cortical area would always destroy the function in question completely and irreversibly. However, the situation is yet more complicated, as the following case studies will demonstrate.
LM had lost most of her capacity to see motion following bilateral posterior brain injury due to sinus venous thrombosis (Rizzo, Nawrot, & Zihl, 1995; Zihl, von Cramon, & Mai, 1983; Zihl, von Cramon, Mai, & Schmid, 1991). She reported, however, somehow “seeing” objects in motion, provided that (1) only one stimulus was moving, (2) the speed of the moving stimulus did not exceed 6 degrees per second, and (3) objects were moving either horizontally or vertically. This “residual” movement vision could either constitute incomplete injury to V5 (the “visual motion” area) or be accounted for by other visual areas. The measurement of brain activity during the processing of moving visual stimuli in LM showed no evidence of activation of V5 in either hemisphere. Somewhat surprisingly, activation was observed in another visual area (V3) and in the superior parietal cortex (Brodmann’s area 7). Both areas, however, are not known to be “functionally specialised” to process visual motion signals and are not activated in normal subjects in the same experimental conditions, but are the likely candidates for LM’s residual movement vision (Shipp, de Jong, Zihl, Frackowiak, & Zeki, 1994; Zeki, 1991). Thus, movement vision is possible without V5, although under extremely restricted conditions. This “residual” movement capacity did not improve over the years and could not be used by LM to substitute the role of her injured V5, which would have reduced her severe daily visual handicaps. Nevertheless, LM learned efficient strategies to cope with her extraordinary visual disorder, mainly by avoiding conditions in which moving stimuli dominated or interfered with her activities.
DF, a patient reported by Milner et al. (1991), suffered a severe visual deficit of form recognition following bilateral posterior brain injury due to asphyxia while taking a shower as a result of a faulty gas water heater. She had great difficulties in discriminating, for example, simple shapes and line orientations. Despite poor performance in these tasks, she had little difficulty in everyday visually guided activities such as opening doors, shaking hands, eating meals, reaching out accurately for and grasping objects differing in form, size and orientation. The authors hypothesised that the preserved visuo-motor ability may depend on routes still functioning from the occipital lobe, where the analysis of visual forms is performed, to neural mechanisms in the parietal lobe that control visually guided movements of the hand and fingers. Explicit visual form perception and recognition is therefore not a crucial prerequisite for an appropriate visual guidance of hand and finger movements. In contrast to LM, who did not benefit from her residual visual motion perception, DF certainly could make use of her “residual” visual form processing capacity in her daily life activities.
Certainly, nobody would interpret the use of spared or substituted visual functions in these two cases as recovery (although it led to functional improvement). Yet, these and similar observations underlie the need for an accurate and detailed analysis of lost, impaired, spared, and substituted visual functions. Otherwise sparing or substitution of function could easily be confounded with recovery of function, especially if systematic practice is required to reveal a spared or substituted visual capacity. Systematic practice might be particularly important to reveal visual capacities in cases with denial of preserved vision (so-called negative Anton syndrome) as well as in cases with a reduction of initiative and self-generated activities due to concomitant depression or reduced motivation (e.g., Feibel & Springer, 1982; Richards & Ruff, 1989; Van de Weg, Kuik, & Lankhorst, 1999). The sites and sizes of brain lesions differ, of course, among patients, but this may not be reflected by the (initial) severity of a single visual deficit or a pattern of visual deficits. Recovery of visual function as well as functional improvement through compensation may, however, depend on the integrity of brain structures beyond the visual cortex and on fibre pathways interconnecting these structures. Thus, knowledge about the networks subserving complex visual capacities, which also include the involved cognitive components, is important in interpreting cerebral visual dysfunction as well as spontaneous recovery and improvement after practice.
Another difficulty arises from the fact that patients cannot (and must not) be kept in a “controlled” constant environment as animals can. Consequently, any kind of improvement of function can in principle also be attributed to confounding “environmental” variables. Finally, how much time should a brain function be given to recover “spontaneously”, and how long should treatment be continued before one can reliably state that no (further) recovery or spontaneous adaptation can be expected? If systematic intervention is started early after brain injury and the function in question returns (partially or completely) the primary and most obvious explanation is that the improvement might also have occurred without systematic intervention. This is a serious argument, but not easy to dismiss, as Poppelreuter (1917/1990) has already noted. Sceptics may even argue that even if treatment starts several weeks or even months after the onset of a functional deficit, an improvement after systematic practice may still represent spontaneous recovery. One possible way of avoiding this problem is to monitor the effect in the experimental group by using a control group. Although this seems to be an ideal methodological approach, one still faces the problem of heterogeneity of brain injury and the resulting differences in functional consequences as well as of controlling for environmental influences. For the patient it is, of course, irrelevant why improvement has occurred as long as it does occur and the outcome is beneficial. For the researcher, however, it is not irrelevant. There is agreement that the adoption of a method of treatment should be based on an underlying theoretical rationale and on the control of non-specific factors (e.g., motivation, emotional state, social support; Robertson, 1994). These factors may impair or enhance the improvement, although they do not represent and cannot substitute specific treatment procedures.
Thus, it seems that rehabilitation research in neuropsychology is a very laborious and difficult task, for which no satisfactory design exists. At the same time it is extremely risky because success cannot be guaranteed, even after a high expenditure of time, resources and energy. Of course, reports on negative findings are just as important as reports on positive outcomes (Barlow & Hersen, 1985), not only for methodological reasons, but also because it allows for the extraction of criteria for making a valid decision about the efficacy of a particular treatment procedure in scientific and pragmatic (i.e., ecologic) terms. When developing and proving new methods, one can hardly predict their potential significance for rehabilitation at the same time. What is possible, however, is to plan, a priori, the development and evaluation of treatment methods, as well as to define patient eligibility criteria and select appropriate outcome measures in the context of behavioural benefit (Baddeley, Meade, & Newcombe, 1980). Using such measures allows the evaluation of treatment-related functional improvements in terms of whether they increase independence and life quality. This is not only important from the viewpoint of rehabilitation research but is also essential for the motivation of patients. The earlier the patient is aware of an improvement in everyday-life activities, the higher will be their motivation to co-operate and the earlier the patient will become an expert on the specific individual difficulties, and how to cope with them.
Studying the recovery of brain function as well as the mechanisms underlying substitution and compensation is not only of importance for neuropsychological rehabilitation but also contributes substantially to the understanding of the functional organisation and reorganisation of the brain and, thus, of brain plasticity. The better we understand dynamic brain– behaviour relationships as well as the potentials of brain plasticity and its underlying processes, particularly in pathological conditions, the more success w...