![]()
Part I
The Americas
Paul G. Shekelle
The continents of North and South America and their proximate islands make up the World Health Organization region of the Americas—an area that exceeds 16 million square miles and extends 8700 miles from north to south. The geography encompasses every extreme: from arctic tundra in the north, through deserts and plains, vast mountain ranges, and large river basins, to tropical rainforests in the south. The combined population of the 35 countries and 24 dependent territories that make up the Americas is more than 1 billion. The population is as demographically, culturally, and economically diverse as the landscape and climate, and includes those in the wealthiest nations of the world, such as the United States and Canada, along with those in some of the poorest, such as Haiti.
Authors from nine countries from the region—Argentina, Brazil, Canada, Chile, Guyana, Mexico, Trinidad and Tobago, the United States, and Venezuela—have contributed to this book, and the overall message is that there is a broad range of possible future innovations and reforms. While the discussion is expansive and each chapter has its own particular focus, shifts in global trends in demographics, economics, and technology mean that there are a number of shared concerns. These include improved training and education (Trinidad and Tobago and Brazil), reforms to health system financing (Chile, Mexico, and Argentina), primary and mental healthcare (Venezuela and Guyana), and the importance of developing patient-oriented systems (Canada and the United States of America).
Concerning potential improvements in training and education, Walter Mendes, Ana Luiza Pavão, Victor Grabois, and Margareth Crisóstomo Portela describe a Brazilian distance education training program designed to improve patient safety and increase research, with an emphasis on collaboration. Claudine Richardson-Sheppard describes ways in which nurse education in Trinidad and Tobago could be improved with the introduction of competency-based training, particularly when it comes to leadership roles.
With regard to how care is paid for, Oscar Arteaga describes Chile’s struggle to create a more fully integrated health insurance system, while Hugo Arce, Ezequiel García-Elorrio, and Viviana Rodríguez home in on the goal of achieving universal healthcare coverage through the targeting of priority populations in Argentina. Jafet Arrieta, Enrique Valdespino, and Mercedes Aguerrebere describe how Mexico might use conditional cash transfers and universal healthcare coverage to tackle the growing burden of non-communicable diseases.
In Venezuela, Pedro Delgado, Luis Azpurua, and Tomás J. Sanabria present an innovation using training and technology to improve primary care in rural clinics. William Adu-Krow, Vasha Elizabeth Bachan, Jorge J. Rodríguez Sánchez, Ganesh Tatkan, and Paul Edwards describe a shift from institutional care to community care when it comes to treating patients with psychological disorders in Guyana.
In Robert H. Brook and Mary E. Vaiana’s radical vision of the future, the U.S. health system has been completely reoriented and adopts a patient-focused approach, with all social and health services integrated. Anne W. Snowdon, Charles Alessi, John Van Aerde, and Karin Schnarr also look forward to a more personalized health system in Canada, where all medical information is accessible and transparent, and health decisions can be made by the informed consumer.
Thus, in the Americas, a wide range of potential future innovations is envisioned, at different stages of development, and influencing care from specialized populations to the entire country. These aggregate to a set of remarkable visions, some of which are more speculative, and others more grounded in the present.
![]()
1
Argentina
Achieving Universal Coverage
Hugo Arce, Ezequiel García-Elorrio, and Viviana Rodríguez
CONTENTS
Argentinian Data
Background
Healthcare Organizations
Human Resources
Twenty-First-Century Health Initiatives
Proposed Health System Reforms
Achieving Universal Coverage
Conclusion
Argentinian Data
| • Population: 43,847,430 • GDP per capita, PPP: $19,934.4 • Life expectancy at birth (both sexes): 76.3 years • Expenditure on health as proportion of GDP: 4.8% • Estimated inequity, Gini coefficient: 42.7% |
|
Source:All data are from the World Health Organization and World Bank. Latest available data used as at October 2017.
GDP = Gross Domestic Product
PPP = Purchasing Power Parity
Background
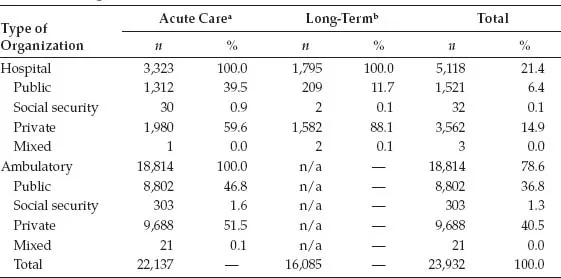
Argentina, like most countries, is in the process of epidemiological and demographic transition. Argentina’s population is largely urbanized (about 80%), and around 32.2% of the population is impoverished. Urbanized areas are served by both ambulatory and hospital services—including public and private, for profit and non‑profit (Table 1.1).
TABLE 1.1
Healthcare Organizations
Source:Ministerio de Salud [Argentina]. (n.d.). Sistema Integrado de Información Sanitaria Argentina. Retrieved from https://www.msal.gob.ar.
Note:n/a = not applicable.
aAll types of organizations with and without admission services, with the exception of centers for geriatric care.
bMight include some mental health and addiction centers.
During the last 2 years, there has been a marked increase in epidemic outbreaks of dengue, Zika, chikungunya, and even yellow fever due to the increase in population and displacement of their common source, the Aedes aegypti mosquito, whose natural reservoir is the jungle of the Mato Grosso. Preventive strategies are multipronged and include education as well as the elimination of the insects and their habitats. Low-income populations in the north and center of the country, where Triatoma infestans (vinchuca) transmit Chagas disease, are particularly vulnerable. Malaria cases, however, are uncommon in the north of the country, as a result of an intense campaign deployed in the 1940s and 1950s.
Chronic non‑communicable diseases (NCDs), such as obesity, diabetes, hyperlipidemias, hypertension, and chronic obstructive pulmonary diseases (COPDs), are simultaneously becoming increasingly common in urban populations. This has forced a shift in urban primary care services’ traditional emphasis on acute and infectious disease control to the management of chronic conditions.
High maternal mortality rates persist in Argentina, due to the prevalence of unchecked chronic conditions, adolescent pregnancies, and illegal abortions, and despite the fact that more than 97% of births occur in hospitals. In 1990, as a signatory to the United Nations (UN) Millennium Development Goals, Argentina committed to reducing its maternal mortality rate by 75%, aiming to reach 1.3 deaths per 10,000 live births by the year 2000. However, the rate is currently 3.2%, with abortion a leading cause of maternal death, especially among teenagers. An estimated 500,000 illegal abortions are carried out every year.
Healthcare Organizations
Argentina has 3300 acute care hospitals, of which 1300 are public and 2000 are private. There are approximately 134,000 beds: 73,500 (55%) public beds and 60,500 (45%) private beds. However, over the past 25 years, the total number of beds per 1000 inhabitants has decreased: from 4.5 in 1995 to 3.1 in 2016. These figures do not take into account the numbers of geriatric patients currently hospitalized, which increases the number to 4.9 per 1000 (Arce, 2010). Several studies indicate that despite superior capacity, public hospitals account for less than 40% of the current system’s resources. There are also 1800 geriatric institutions with about 80,000 beds where the public patients account for less than 12% of the total. There has been a notable increase in the number of outpatient clinics over the last three decades: in total, there are 18,800 establishments with 8,800 public centers primarily concerned with general primary care, and 10,000 private diagnostic and specialis...