Healthcare Affordability
Motivate People, Improve Processes, and Increase Performance
- 158 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
Healthcare Affordability
Motivate People, Improve Processes, and Increase Performance
About This Book
Healthcare Affordability: Motivate People, Improve Processes, and Increase Performance applies the Theory of Affordability across the Healthcare Enterprise. Affordability is realized when the Value delivered exceeds the Patient's requirements, while the expense for the quality resources required to deliver that Value is at a Cost less than the revenue received from the competitive pricing applied to the care.
The aim of healthcare affordability is to attain performance excellence in all areas across the entire Healthcare Enterprise. The Healthcare Enterprise involves 5 types of providers: Healthcare Providers, Medicine and Pharmaceutical Providers, Machine and Device Providers, Service and Supplier Providers, and Insurance and Payment Providers. Obviously, one key focal point of healthcare affordability is affordable healthcare, a condition that has been chased for decades, but has yet to be achieved.
This book provides a useful framework and foundation for any organization to pursue and achieve Affordability. Although there are many methods used to accomplish performance improvement, this approach has been proven successful with many organizations. It integrates strategic vision and direction, with operational goals and objectives and tactical targets and tasks. This book also provides a leadership strategy and structure for change and transformation, and a designed plan to execute an 18-month implementation program.
Features:
-
- Affords patients and providers a better, faster, safer, and more affordable and profitable experience and approach
- Offers solutions for current state dilemmas, and provides a framework for future state success
- Increases the speed of delivery, improves the quality, and decreases the cost of care
- Provides methods and tools for linking and integrating strategic, operational and tactical goals
Healthcare Affordability: Motivate People, Improve Processes, and Increase Performance provides readers with methods and means for solving the complex problem of affordable healthcare.
Frequently asked questions
chapter one
Making the case for Healthcare Affordability
- Why isn’t healthcare becoming more affordable?
- How can healthcare become more affordable?
- What can be done to achieve Healthcare Affordability?
- Who needs to be involved to accomplish Healthcare Affordability?
Affordable healthcare and Healthcare Affordability
- According to Forbes (Leah Binder), “The Five Biggest Problems in Healthcare Today”1; (1) Too much unnecessary care, (2) Avoidable harm to patients, (3) Billions of dollars are being wasted, (4) Perverse incentives on how we pay for care, and (5) Lack of transparency
- From HealthPAC online2: The issues to address in the reform of the healthcare system: affordability, portability, accessibility
- CNN’s report on “America’s 9 Biggest Health Issues”3: Doctor shortage, hospital errors and infections, antibiotic resistance, more do-it-yourself healthcare (apps and technology), food deserts, caregivers for the aging population, the cost of Alzheimer’s, marijuana, and missing work–life balance
- Healthcare Business and Technology published “Top 10 Issues impacting the Healthcare Industry in 2016”4: mergers, drug prices, mobile care, cyber security concerns over medical devices, money management, behavioral health moves to front of stage, community care collaboration, new databases, welcome biosimilars, and medical cost mystery.
- The Medical Examiner5 tells us: Congress Has Forgotten America’s Biggest Healthcare Problem—The critical question is not who gets care, and who doesn’t, but how it’s delivered.
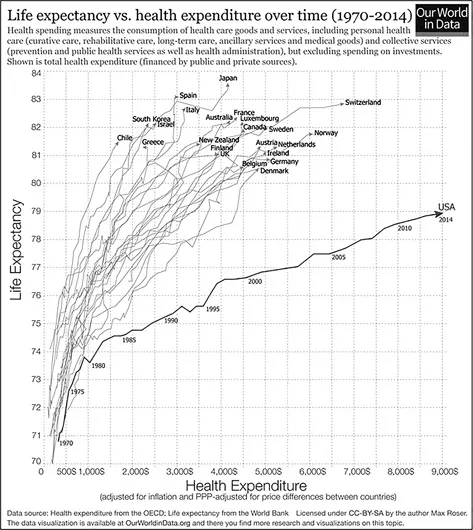
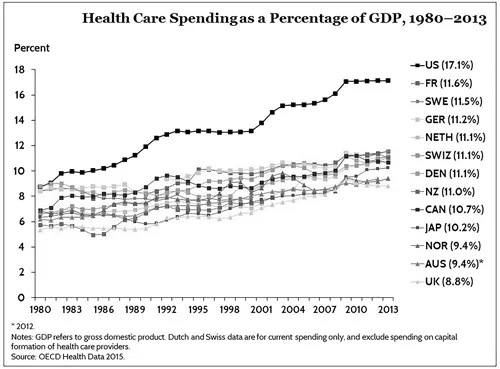
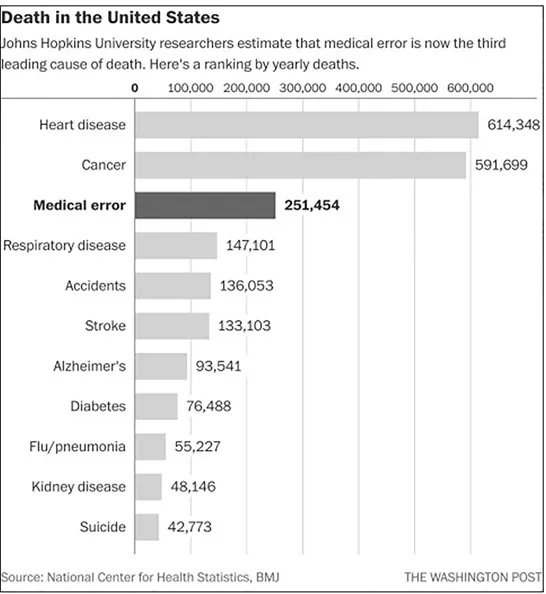
- The Physicians for a National Health Program6 claim: (1) Americans pay way, way, way more for health care than anyone else. (2) We pay doctors when they provide lots of care, not when they provide good health care. (3) Half of all health care goes toward 5% of the population. (4) Our health insurance system is the product of random WWII-era tax provisions. (5) Insurance companies have small profit margins. (6) Getting health care in the United States is dangerous (medical errors). (7) One third of health care spending isn’t helping make Americans healthier (i.e., $765 Billion). (8) Obamacare is not universal health care.

Some personal observations and case-study perspectives
- Waiting: Patients waiting, patient care givers waiting, healthcare providers (i.e., physicians, nurses, technicians, assistants, and aides) waiting, machines and devices waiting to be utilized, with materials and supplies waiting to be used.
- Excessive motion: Systems designed to cause workers to expend energy in movement and motion, in order to, “get the job done.” For example, nurses having to spend a great deal of their time going to storage locations to get materials and supplies to treat patients.
- Medical defects: Being the third leading cause of death, flaws, and weaknesses in systems as a result of inconsistencies and imperfections of processes and procedures.
- Lots of meetings, with lots of people.
- Lots of charts and spreadsheets, with lots of data.
- Lots of emails, copying lots of people.
- An inherent “shame and blame” culture, trying to find out “who did it.”
- “Busy-ness” with lots of effort and lots of activity.
- A cautious, defensive behavior by those directly involved.
- A Physician-centered System based primarily on Physician Decisions and Physician Schedules.
- A Revenue Cycle Focus putting money as the top priority for the organization.
- …and lots more.
- Assign and task individual with improvement activities (i.e., more accountability for “fixing”).
- Increased awareness of focus on quality.
- More performance feedback has been emerging.
- New policies and procedures focused on “fixing the problem.”
- Some incentives for resolving quality issues.
- Punishment and penalties continued to prevail.
- The emphasis to promote good will emerged.
- The attitude to work harder to do better was embraced.
- Four common themes for poor performance (Roger K. Resar, Making Noncatastrophic Health Care Processes Reliable: Learning to Walk before Running in Creating High-Reliability Organizations...
Table of contents
- Cover
- Half Title
- Title Page
- Copyright Page
- Table of Contents
- Preface
- Chapter 1 Making the case for Healthcare Affordability
- Chapter 2 Healthcare Affordability defined
- Chapter 3 Healthcare Affordability applied
- Chapter 4 The strategic dimension
- Chapter 5 The operational perspective
- Chapter 6 The tactical reality
- Chapter 7 First and foremost, assess the situation
- Chapter 8 Design the solution and plan for success
- Chapter 9 Implement improvements
- Chapter 10 Maintain and sustain the results … continuously improve
- Chapter 11 Enterprise wide responsibilities
- Chapter 12 The end … start now
- Appendix A
- Appendix B
- Appendix C
- Appendix D
- Index