Non-Invasive Instrumentation and Measurement in Medical Diagnosis, Second Edition discusses NIMD as a rapidly growing, interdisciplinary field. The contents within this second edition text is derived from Professor Robert B. Northrop's experience teaching for over 35 years in the Biomedical Engineering Department at the University of Connecticut. The text focusses on the instruments and procedures which are used for non-invasive medical diagnosis and therapy, highlighting why NIMD is the preferred procedure, whenever possible, to avoid the risks and expenses associated with surgically opening the body surface. This second edition also covers a wide spectrum of NIMD topics including: x-ray bone densitometry by the DEXA method; tissue fluorescence spectroscopy; optical interferometric measurement of nanometer tissue displacements; laser Doppler velocimetry; pulse oximetry; and applications of Raman spectroscopy in detecting cancer, to name a few. This book is intended for use in an introductory classroom course on Non-Invasive Medical Instrumentation and Measurements taken by juniors, seniors, and graduate students in Biomedical Engineering. It will also serve as a reference book for medical students and other health professionals intrigued by the topic. Practicing physicians, nurses, physicists, and biophysicists interested in learning state of the art techniques in this critical field will also find this text valuable. Non-Invasive Instrumentation and Measurement in Medical Diagnosis, Second Edition concludes with an expansive index, bibliography, as well as a comprehensive glossary for future reference and reading.
- 500 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
Non-Invasive Instrumentation and Measurement in Medical Diagnosis
About this book
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
Topic
MedicineSubtopic
Biotechnology in Medicine1Introduction to Noninvasive Medical Measurements
1.1Definitions of Noninvasive, Minimally Invasive, and Invasive Medical Measurements
In this chapter, let us attempt to reach consensus about what we mean by noninvasive (NI) medical measurements. Any measurement system that does not physically breach the skin, or enter the body deeply through an external orifice is truly NI. Thus, the measurement of body temperature with a thermometer in the mouth, rectum, or ear canal is considered NI, as is the use of an otoscope to examine the outer surface of the eardrum. Similarly, the use of the ophthalmoscope and slit lamp which shine light in the eyes to examine the retina and the cornea and lens, respectively, is considered NI procedures. The transduction of sounds from the body surface (from the heart, breath, otoacoustic emissions, joint sounds, etc.) is truly NI, as is the recording of electric potentials on the skin from internal sources such as the heart (ECG), skeletal muscles (EMG), brain (EEG), etc. Medical imaging techniques such as x-ray, x-ray tomography (CAT scan), ultrasound, magnetic resonance imaging (MRI), positron emission tomography (PET), etc. are NI; they do involve the input of energetic radiation into the body, however, which generally carries low risk when proper energy levels and doses are observed.
Much can be learned from blood samples; namely, ion concentrations, red blood cell density, white blood cell density, the concentrations of certain hormones, antibodies, cholesterol, drug concentrations, DNA type, pathogens, chemical indicators of chronic diseases, etc. The drawing of small blood sample, say <1 cm3, from a superficial vein by a needle and syringe or a lancet is considered to be a minimally invasive procedure, requiring sterile technique.
Endoscopy is a technique for visualizing tissues deep within the body yet topologically on the outer surface of the body. An example is bronchoscopy, where a bronchoscope is inserted through the mouth and larynx, into the trachea and bronchial tubes of the lungs to permit visualization of their surfaces and the surfaces inside larger alveoli. Another endoscope is the cystoscope which is inserted into the urethra to inspect the ureter, the prostate, and the inside of the bladder. Many other types also exist (Section 2.3). As a rule, endoscopes require sterile technique, and in most cases, local or general anesthesia; I consider them to be moderately invasive instruments, and endoscopies moderately invasive procedures.
Some endoscopes are used invasively, such as laparoscopes, which are inserted into the abdomen through a small incision in the wall of the abdomen, chest, or back. They are used to examine the outsides of the internal organs (bladder, gall bladder, intestines, kidneys, liver, lungs, spine, spleen, uterus, etc.) for tumors, infections, damage from trauma, etc. Another invasive procedure, for example, is cardiac catheterization with a fiber optic endoscope in order to view heart valves.
One can argue that there are fuzzy classification boundaries separating NI, minimally invasive, moderately invasive, and invasive diagnostic procedures. Anyone who has undergone a colonoscopy or proctoscopy may be quick to argue that they are more invasive than minimally invasive diagnostic procedures, considering the preparation, medication (analgesia or anesthesia), and discomfort involved. Thus, we argue that invasiveness should be assessed on a four-level (two-bit) scale, that is, levels 0–3.
This text is about the instruments and measurement systems used in making modern, non-invasive medical diagnoses (NIMDs). Some of the instruments and systems described are well-established, Food and Drug Administration (FDA)-approved systems; others are prototype systems that eventually may prove safe, medically and cost-effective. It is important for the reader to know where the field of NI diagnostic instrumentation is headed, as well as its present status. Its evolution is rapid, fueled by the advances in information processing and storage, as well as in the fields including photonics, molecular biology, and medical physics.
Throughout the history of medicine, up to the end of the nineteenth century, most medical diagnoses were necessarily NI. The physician used his or her eyes to observe skin lesions, and inflammation in the nose, throat, gums, ears, and skin. Tactile senses in the physician’s hands were used to feel skin temperature, edema, swelling due to infection, lumps under the skin, etc. The physician’s ear was used to listen to breath, bowel, and heart sounds. The odors of infection was sensed by the physician’s nose. Exploratory surgery was seldom done because of the risk of shock due to pain and blood loss, and danger of infection.
Today, considerable emphasis is on the use of NI diagnosis in health maintenance and emergency medicine. Most of it can be carried out on an outpatient basis, and carries little risk of infection or complications which would add to the cost the patient’s health maintenance organization (HMO) must pay. On the other hand, certain NI instruments, such as the various medical imaging systems, are very expensive to build and maintain and their use fee is commensurately large. Indeed, NI diagnostic procedures, including imaging systems, have been accused of driving up the cost of health maintenance and care. The effective but simple NI, level 0 instruments such as the electrocardiograph, the spirometer, and the slit lamp and their use certainly are not culprits in this respect. The advantage of being able to see tumors in the middle of soft tissues such as the brain, lungs, liver, spleen, and breasts will continue to drive the need to improve the resolution of expensive imaging systems, and to ensure their use where indicated.
1.2Modalities of NI Instrumentation
NI medical instruments can be broadly classified between those passive systems that put no energy into the body, and those that input some form of radiation energy, for example, microwaves, visible and UV light, x-rays, γ-rays, sound and ultrasound, and measure what energy is either absorbed, reflected, or transmitted at different wavelengths or frequencies. Among the purely passive systems, we have the well-known electrical measurements based on active nerve and/or muscle membranes. These include time-varying electrical potentials recorded from the skin surface from the heart (ECG), brain (EEG), muscles (EMG), ears (electrocochleogram [ECocG]), and eyes (EOG and ERG). Sounds from the body’s interior can also be recorded from the skin surface, including sounds from the heart valves, pericardium (friction rub), blood vessels (bruit), lungs, bronchial system, pleural cavity, eardrums (spontaneous otoacoustic emissions), joints, etc. Body temperature can be sensed from the infrared radiation from the eardrum, or by physically measuring the temperature of the saliva and tissues under the tongue, or the temperature in the rectum by a liquid-in-glass thermometer, or a thermometer based on a thermistor or platinum resistance element (resistance temperature detector [RTD]). Tissue oxygen and carbon dioxide partial pressures (pO2 and pCO2) can be measured transcutaneously with special chemical electrodes. The only energy put in by endoscopes is white light required to visualize or photograph the tissue being inspected. Blood pressure can be measured noninvasively by Korotkoff sounds emitted by the brachial artery as the pneumatic pressure in a sphygmomanometer cuff is slowly reduced, allowing blood to surge into an artery.
Just about every other physiological modality that can be measured noninvasively requires some small input of energy. An important class of NI imaging systems uses pulsed ultrasonic energy. The energy level of the input ultrasound is made low enough to avoid tissue-destroying cavitation or heating. Other NI, nonimaging, diagnostic systems that use continuous-wave (CW) ultrasound include Doppler blood velocity probes and Doppler probes used to sense the fetal heartbeat or detect aneurisms.
Electromagnetic radiation includes radio-frequency electromagnetic waves, THz waves, infrared (IR), visible, and ultraviolet, as well as x-rays and gamma rays (Figure 1.1). The photons from UV radiation, x-, and gamma rays have sufficient photon energy (hν) to knock atomic electrons out of their inner orbits and rupture certain molecular bonds, causing DNA mutations, etc.; UVB, x-, and gamma rays are called ionizing radiations because of the potential destruction they can cause to biomolecules as the result of ionization of water and other molecules. Thus, the use of NI instruments that emit ionizing radiation is not without some small health risk. UVB photons do not penetrate the skin deeply; hence, UV damage to skin can include reddening (burns) and the initiation of various types of skin cancers. The corneas and lenses of eyes given excessive UVB radiation can develop cataracts. X- and gamma ray photons, on the other hand, can penetrate the body deeply, causing cell damage in the organs. A high-energy x-ray photon can directly damage a DNA molecule, leading to a cellular mutation if not internally repaired by the cell. If a photon-dislodged electron strikes a water molecule, it can create a free radical. The estimated lifetime of a free radical is ∼10 µs, which means it can drift and encounter a DNA molecule, producing indirect damage as stable molecular configurations are restored. Note that we are mostly concerned with electromagnetic ionizing radiations in this text. Certain radioisotopes used in medical imaging and in cancer therapy emit energetic alpha particles (He nuclei), beta particles (electrons), or neutrons. These energetic particles can also generate free radicals and cause DNA damage, and initiate cell death by apoptosis.
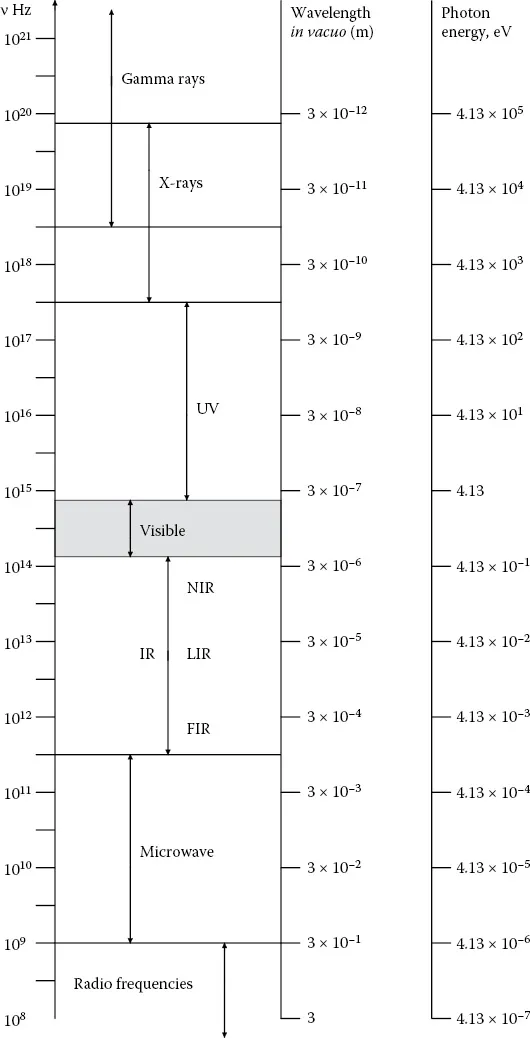
Figure 1.1Electromagnetic spectrum ranges that find application in medical diagnosis. Photon energies in electron volts at a given wavelength are given in the right-hand column.
X-ray machines of all sorts, bone densitometers, and CAT and PET scanners thus carry a small risk of inducing cancer, including leukemia, in the patient. However, most healthy persons absorb far more ionizing radiation in the form of 5.5 MeV alpha particles from the radioactive breakdown of inhaled, naturally occurring, radon gas (e.g., 222Rn) than they do from x-rays. Note that 36 radioisotopes of 222Rn have been characterized, with atomic masses ranging from 193 to 228. 210Pb is formed from the decay of 222Rn.
Other NI instrumentation systems such as impedance plethysmographs, pass low levels (in the microamp range) of alternating current (AC) in the frequency range from 25 to 100 kHz through the tissues being studied. The input of this current is apparently without risk; it is way...
Table of contents
- Cover
- Half Title
- Series Page
- Title Page
- Copyright Page
- Dedication
- Contents
- Preface
- About the Author
- Acronyms and Abbreviations
- 1. Introduction to Noninvasive Medical Measurements
- 2. Visual Inspection of Tissues with Certain Endoscopes and Other Optical Devices
- 3. Noninvasive Diagnosis Using Sounds Originating from within the Body
- 4. Measurement of Electrical Potentials and Magnetic Fields from the Body Surface
- 5. Noninvasive Measurements of Blood Pressure
- 6. Body Temperature Measurements
- 7. Noninvasive Blood Gas Sensing with Electrodes
- 8. Tests on Naturally Voided Body Fluids
- 9. Plethysmography
- 10. Pulmonary Function Tests
- 11. Measurement of Basal Metabolism
- 12. Ocular Tonometry
- 13. Noninvasive Tests Involving the Input of Audible Sound Energy
- 14. Noninvasive Tests Using Ultrasound (Excluding Imaging)
- 15. Noninvasive Applications of Photon Radiation (Excluding Imaging)
- 16. A Survey of Medical Imaging Systems
- 17. Innovations in Noninvasive Instrumentation and Measurements
- 18. Introduction to Noninvasive Therapies
- Bibliography
- Glossary
- Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Non-Invasive Instrumentation and Measurement in Medical Diagnosis by Robert B. Northrop in PDF and/or ePUB format, as well as other popular books in Medicine & Biotechnology in Medicine. We have over 1.5 million books available in our catalogue for you to explore.