1 The Red Eye: Basic Algorithm on How to Differentiate Main Conditions from Each Other
Amy-lee Shirodkar
Key Points
1.Appreciate the difference between causes of a red eye that are urgent vs non-urgent
2.Causes of a red eye tend to involve the anterior segment
3.Associated symptoms and history will help localise the problem
4.Lid eversion and checking for corneal sensation are often missed
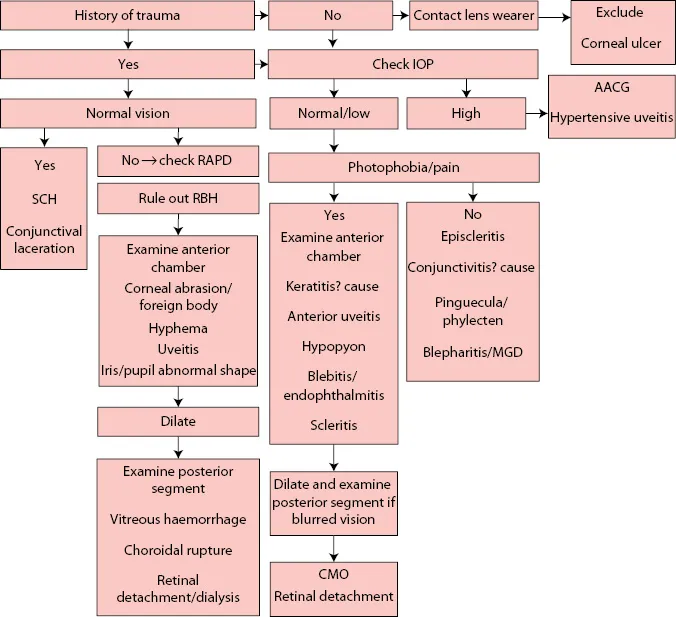
Diagram of Algorithm
Referral and Presentation
This is the commonest and least useful presentation of any ophthalmic condition. It can range from the trivial to the potentially blinding and even life-threatening. As such patients may present with a red eye for different reasons and at different time periods depending on a thousand factors ranging from a worry at how they look to a deep seated fear of going blind, with factors such as work, booked holidays or childcare arrangements resulting in great variations as to when a patient with the same condition may present to your department. There may be associated pain, tenderness, photophobia or foreign body sensation – depending on the cause. A red eye might be associated with blurred vision or indeed there may be no visual disability whatsoever. There may be no true emergency, but the eye may just look alarming to friends and family, such as classically with a subconjunctival haemorrhage. Either way, a patient has presented to you with a red eye but you should, through triage, see the true emergencies first: penetrating trauma, acute angle closure glaucoma (AACG) or endophthalmitis for example. Triage is fundamental here more than anywhere.
Knowing the patient’s medical history may immediately guide you toward the likely diagnosis, especially if they suffer ocular conditions that have a high risk of recurring such as uveitis, marginal keratitis and herpetic disease for example, or have recently had eye surgery. Systemic conditions with known ocular associations should guide thought processes such that patients with rheumatoid arthritis for example may be more likely to present with corneal melting and scleritis than a patient who has osteoarthritis. Taking a drug history may shine the light on a reason for extensive subconjunctival haemorrhage such as an anticoagulant or use of a topical medication causing allergy. Other important questions to ask in the history include: contact lens wear, potential causes of trauma, recent surgery, previous ocular conditions and past medical history including atopy.
Differential Diagnosis
The eye may appear red for two reasons: haemorrhage or inflammation. Haemorrhage can appear spontaneously such as with subconjunctival haemorrhage after trauma (blunt, penetrating or iatrogenic) or secondary to infections such as viral conjunctivitis. A red, injected eye with varying pain may be due to inflammation or infection of one or more components of the eye. There are two main ways to sort out the causes of a red eye in your mind. One method is to classify causes by anatomy (see Table 1.1) the second by severity and likelihood of permanent visual injury (see Table 1.2). Ultimately there are only a handful of true ophthalmic emergencies that will cause permanent sight loss if not treated urgently: orbital cellulitis, retrobulbar haemorrhage, AACG, globe disruption (through trauma or corneoscleral melting) and endophthalmitis. The other eye conditions can be classified as urgent or non-urgent depending on the probability of causing permanent irreversible blindness.
| Table 1.1: Causes of Red Eye Diagnoses Depending on Affected Area |
| Affected Area | Causes of Red Eye |
| Eyelids | Cellulitis – orbital, preseptal Blepharitis Molluscum Herpes zoster ophthalmicus Entropion, ectropion, trichiasis |
| Conjunctiva | SCH Conjunctivitis – infective, allergic, autoimmune |
| Sclera/episclera | Scleritis, episcleritis |
| Cornea | Keratitis Infective – viral, bacterial, acanthamoeba Inflammatory – marginal keratitis, peripheral ulcerative keratitis, superior limbic keratitis Corneal abrasion, erosion, exposure Neuropathic causes of abrasion or ulceration |
| Anterior chamber | Uveitis, hyphema |
| Raised IOP | Glaucoma – AACG, secondary causes |
| Lens | Phacolytic, phacomorphic, phacoanaphylactic glaucoma |
| Others | Carotid cavernous fistula, malignant lesions, retrobulbar haemorrhage |
| Trauma | Laceration – eyelids, cornea, sclera, IOFB |
| Table 1.2: Triage of Red Eye Depending on Cause |
| Emergency | Urgent | Non-Urgent |
| Acute angle ... |