- 104 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
About this book
This brand-new revision aid has been designed specifically to help medical students and early post-graduate doctors learn and remember pertinent information about various neurological conditions through pictorial representation, and will be invaluable throughout medical studies and particularly useful in the pressured run-up to final and post-graduate examinations.
The highly-structured information is presented in a consistent, double-page format. Each condition is represented by a characterful and memorable visual mnemonic, accompanied by a concise, high-yield review covering definition, aetiology, epidemiology, presentation, investigation, management, complications and prognosis. Over 40 common conditions are included, organized alphabetically for ease of reference.
Neurology is often viewed as a challenging subject to learn. By utilising visual imagery to aid memory and recall of important information, the author brings a refreshing new approach to knowledge consolidation.
Tools to learn more effectively

Saving Books

Keyword Search

Annotating Text

Listen to it instead
Information
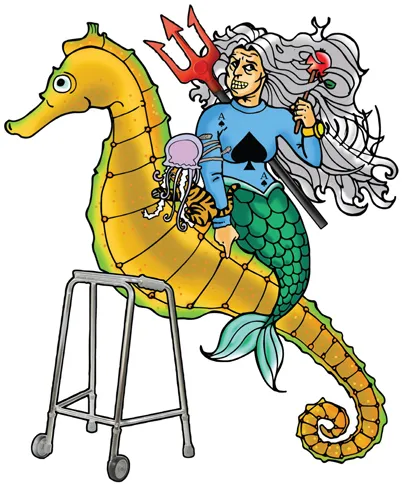
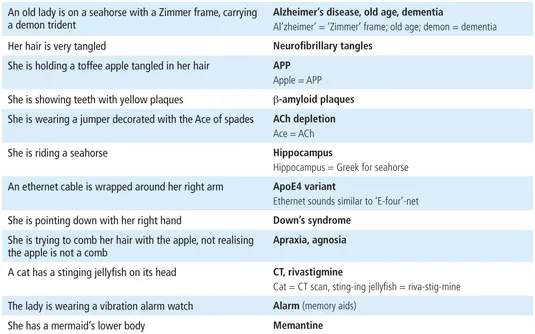
Alzheimer’s Disease
Definition
Aetiology
- Pathophysiology:
- Tau protein (maintains neuronal cytoskeleton) is normally phosphorylated. Tau protein mutation → hyperphosphorylation → tau proteins become unstable and clump together = neurofibrillary tangles → damage neuronal structural integrity. Tangles correlate with dementia severity
- APP is a transmembrane protein (with a role in neuron regulation). Mutation → abnormal APP cleavage → forms β-amyloid; combines into β-amyloid plaques → lead to neuronal death; especially cholinergic fibres (hence why ↓ACh). Starts in the hippocampus, then progresses to the cortex
- Risk factors:
- Age (largest risk factor), prior intellectual level
- Genetics:
- Early onset; autosomal dominant; point mutations in genes associated with amyloid processing: APP, PS1 on chr. 14 and PS2 on chr. 1)
- Late-onset (non-familial); ApoE4 variant
- Down’s syndrome (APP on chr. 21; Down’s = trisomy 21; 3 copies of APP → ↑β-amyloid plaque formation)
Epidemiology
- Most common cause of dementia (60–80% of all dementias)
- Affects 5% of >65 y/o. Incidence ↑exponentially with age
Presentation
- ‘5 As’ presenting in a steady decline. If they occur abruptly, consider vascular dementia:
- Anterograde amnesia: forgetfulness is usually the first presenting sign
- Agnosia: inability to recognise/identify objects despite intact sensory function
- Apraxia: impaired ability to carry out motor activities despite intact muscle strength
- Abnormal executive functioning: impaired planning, organising, abstracting
- Aphasia: language disturbance, typically spared until later
Investigations
- A diagnosis of exclusion; definitively diagnosed only on autopsy
- Bloods: dementia screen; B12, U&E, thyroid function, syphilis serology (if appropriate)
- CT/MRI: may see gross anatomical changes, excludes treatable space-occupying lesions:
- Diffuse cortical atrophy, leading to widened sulci and narrowed gyri
- Hydrocephalus ex vacuo: ventricles enlarge due to brain atrophy, not due to ↑CSF
- Use MMSE and Wechsler adult IQ scale to help assess severity:
- MMSE: <27 qualifies for dementia; however, premorbid intellectual function needs to be taken into account
- Psychometric testing: distinguishes dementia from depression (depressive pseudo-dementia)
Management
- Largely supportive:
- MDT approach is paramount; supportive therapy for patients and family
- Treatment of associated symptoms: depression, agitation and sleep disturbances
- Adaptations: memory aids (diaries, labels), alarms
- Prevent disease progression; start medication if MMSE >12 (if <12, the drug side-effects outweigh the benefits):
- 1st line/mild-moderate: AChE inhibitors, e.g. rivastigmine; ↑ACh levels
- 2nd line/moderate-severe: NMDA receptor antagonist (memantine); ameliorates glutamate-induced cytotoxicity
Complications
- Death commonly results from infection, i.e. bronchopneumonia
- Haemorrhagic stroke: β-amyloid can deposit in cerebral blood vessels and weaken them (cerebral amyloid angiopathy)
Prognosis
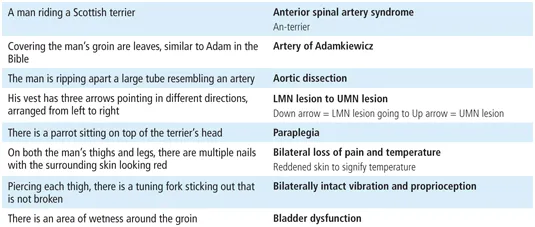
Anterior Spinal Artery Syndrome

Definition
Aetiology
- ASA ischaemia at the level of the spinal cord is known as anterior spinal artery syndrome (or anterior cord syndrome)
- ASA ischaemia at the level of the medulla is known as medial medullary syndrome; it has a different clinical presentation – see below
- Anatomy: the ASA supplies the anterior 2/3rd of the spinal cord and is formed by the anastomosis of the vertebral arteries at the level of the foramen magnum. As the ASA moves down, it receives 6–8 major radicular branches originating mostly from the aorta; the artery of Adamkiewicz (supplies ASA below ~T8) is the largest and most important of these
- Pathophysiology: the formation of the ASA from multiple sources leaves it vulnerable to watershed ischaemia, particularly during aortic occlusion or hypotension. ASA hypoperfusion leads to bilateral disruption of the corticospinal and spinothalamic tracts, with characteristic preservation of dorsal column function (as supplied by the posterior spinal arteries)
- Causes:
- Aortic pathology: aortic dissection, aortic aneurysm, aortic thrombosis
- External compression: herniated disc, neo- plasm, posterior osteophyte
- Thrombotic occlusion of the ASA
Epidemiology
- Spinal cord infarction accounts for approximately 1.2% of all strokes
- Annual incidence: 12/100,000
Presentation
Anterior spinal artery syndrome
- Acute stage: fl paralysis and loss of deep ten- don refl (spinal shock; presents as an LMN lesion), occurs below the level of the lesion, due to involvement of the corticospinal tract:
- Over days → weeks: evolves into spasticity and hyper-refl with an extensor plantar response (UMN lesion)
- Paraplegia: tetraplegia occurs if above C7
- Bilateral loss of pain and temperature at and below the level of injury (as is involvement of the lateral spinothalamic tracts)
- Bilaterally intact vibratory senses, propriocep- tion and 2-point discrimination (intact posterior columns)
- Autonomic dysfunction: orthostatic or frank hypo- tension
- Sexual dysfunction, and/or bowel and bladder dysfunction, depending on the level of the lesion
Medial medullary syndrome
- ASA infarction...
Table of contents
- Cover
- Halftitle
- Title Page
- Copyright Page
- Table of Contents
- Foreword
- Preface
- Acknowledgements
- How to Use this Book
- Abbreviations
- 1 Alzheimer’s Disease
- 2 Anterior Spinal Artery Syndrome
- 3 Ataxia Telangiectasia
- 4 Brown-Séquard Syndrome
- 5 Cavernous Sinus Syndrome
- 6 Charcot–Marie-Tooth Disease
- 7 Cluster Headache
- 8 Creutzfeldt–Jakob Disease
- 9 Encephalitis
- 10 Epilepsy
- 11 Extradural Haematoma
- 12 Facial Nerve Palsy
- 13 Friedreich’s Ataxia
- 14 Frontotemporal Dementia
- 15 Guillain–Barré Syndrome
- 16 Horner’s Syndrome
- 17 Huntington’s Disease
- 18 Hydrocephalus
- 19 Idiopathic Intracranial Hypertension
- 20 Lambert–Eaton Myasthenic Syndrome
- 21 Meningitis
- 22 Migraine
- 23 Motor Neuron Disease
- 24 Multiple Sclerosis
- 25 Myasthenia Gravis
- 26 Myotonic Dystrophy
- 27 Neurofibromatosis
- 28 Normal Pressure Hydrocephalus
- 29 Osmotic Demyelination Syndrome
- 30 Parkinson’s Disease
- 31 Post-Herpetic Neuralgia
- 32 Stroke
- 33 Sturge–Weber Syndrome
- 34 Subacute Combined Degeneration
- 35 Subarachnoid Haemorrhage
- 36 Subdural Haematoma
- 37 Syringomyelia
- 38 Trigeminal neuralgia
- 39 Tuberous Sclerosis
- 40 Von Hippel–Lindau Syndrome
- 41 Wallenberg Syndrome
- 42 Wernicke–Korsakoff Syndrome
- Index
Frequently asked questions
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.4M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app