Treating Psychosomatic Patients: In Search of a Transdisciplinary Framework for the Integration of Bodywork in Psychotherapy offers a conceptual and therapeutic framework for all therapists who have to deal with the psychosomatic 'conflicted' body, as presented in anxiety and depression, stress and burn-out, medically unexplained symptoms and trauma.
The book introduces the transdisciplinary framework 'experiential bodywork' (EBW), drawing on theories and scientific findings drawn from clinical psychology, philosophy, neuroscience, psychotherapy and myofascial therapy. EBW provides a roadmap for a better understanding of the processes that underpin body psychotherapy and body-mind therapies. On a practical level, EBW challenges the therapist to marry the power of psychotherapeutic techniques with the richness of hands-on bodywork and hands-off movement expression. With the 'armoured' body as an entry point, patients learn to feel their body from within and listen to what it tells them. In the sharpness of this awareness they discover a freer way of speaking, moving and being present in the world.
Through EBW, Treating Psychosomatic Patients offers a transdisciplinary, scientifically based framework for the integration of bodywork in psychotherapy, ranging from psychosomatics to trauma, and will be of great interest to psychologists, psychotherapists and counsellors in a variety of settings. EBW also helps somatic therapists,such as physical therapists or osteopaths, to better understand the richness and layeredness of deep bodywork from different psychological, developmental and 'embodied' perspectives.
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
In today’s healthcare system, it is almost standard to map out the broad context in which the patient finds himself. Few people will question the importance of this. How this is best done and for what purpose it should be used in practice, is another question altogether. Academic studies prefer to work with a biopsychosocial model (Engel, 1980). Somatic therapists will therefore not only shed light on the somatic side, but will also consider the patient’s psychological and social environment. In mental healthcare, it is the natural course of events that somatic data are added. Although biopsychosocial classification models, such as the ICF model,1 offer an answer to earlier and one-sided bio-medical approaches, and even though they are now well established (Mahdi et al., 2017; Stucki et al., 2017; Gorostiaga et al., 2017; Linde, 2017; Muschalla et al., 2017), there are obvious weaknesses and shortcomings (Heerkens et al., 2017; Sabbe, 2010).2 Within EBW, we opt for an alternative as a stepping stone.
Towards a transdisciplinary model
Within a transdisciplinary model for the psychosomatic body, there must also be room for development-oriented and process thinking, for the fundamental role of experience and meaning, and for the unconscious.
In summary, the ICF model (WHO, 2002) departs from three perspectives, namely, the human being as an organism (‘the body’), as an acting subject (‘activities’) and as a participating subject in an environment (‘participation’). Here, characteristics, functions and disorders (body), activities and limitations (actions) are distinguished, alongside participation and participation issues. Finally, the ICF model also takes stock of possible influencing factors that are divided into two categories, namely, personal factors and external factors. The latter can consist of an extensive series of subcategories. The personal factors, on the other hand, are identified within the ICF model, but are not really fleshed out in any more detail. Despite the value and application outlined earlier, within EBW, we decide against using the ICF model, but opt for an alternative. Reasons for this include the fact that within the ICF model, there is hardly any room for development-oriented dynamics or process thinking, nor for the fundamental role of experience and meaning, and certainly not for the role of the unconscious as a phenomenon and factor in human functioning. This makes the ICF model too unrefined to use in an integrated approach such as EBW. It is also interesting to note that the ICF model does not deal with possible influencing factors, such as the individual’s personality structure. It is also striking that the patient’s experience is scarcely given any space, although it appears to play a crucial role as a risk factor in the development of functional, somatic syndromes (Henningsen et al., 2007).
The model that we use as an alternative within EBW is partly based on the work of American philosopher Ken Wilber (1949), in which a transdisciplinary vision of the individual’s development is central. This author introduces a number of instruments and concepts, including the Four Quadrant Model and the developmental fulcra. Both are explained for the first time in this chapter. Whereas the ICF model hardly discusses the patient’s world of experience, the family climate and the group dynamics in which he grew up, and certainly not the interactions between these factors, Wilber’s concepts offer a special added value for a development-dynamic view of the individual. However, Wilber’s oeuvre is not always equally undiscussed and has been subject to criticism, such as too little exposure to peer review and too many attempts to integrate fields of knowledge that are so far apart that it threatens to become a ‘theory of everything’. These comments, mainly from academia, should rightly be taken to heart, but mostly relate to the later periods of his oeuvre. The concepts and vision mentioned earlier, which we try to translate within the scope of this book, originate from the early and mid-periods of Wilber’s oeuvre, in which we agree with the academic-scientific attitude that he adopted at that time. In our opinion, this is not only his most productive period, but also his most innovative. Most critics of his work agree on this. The translation to therapy is made in Chapter 7. Here we consider the first concept: the Four Quadrant Model.
The Four Quadrant Model3
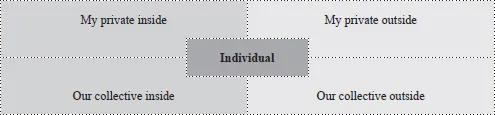
In essence, the Four Quadrant Model (4QM) has a simple basic form.4 The individual is central to four quadrants, each representing a specific and unique aspect of human reality. The model is briefly explained step-by-step as follows. Wilber starts from the observation that each individual has a personal, private side that is his or her own, but is, at the same time, always part of different groups, such as a family, a family and a culture. In other words, we all have a private side and a collective side. So, with our patient in the centre, we first sketch a square with a private upper half and a collective lower half.
In addition, each individual also has an exterior that is visible and tangible and whose contents we can measure and even touch in one way or another.
This measurable exterior is opposite an interior that we can only experience and feel. The inside and outside are represented as a left and a right half of the square in which we just placed the patient in the centre. The interesting thing about the 4QM is that Wilber overlays these four distinct sides or aspects of reality as planes in the model, so that four different combinations or quadrants arise (Figure 1.1). The model then consists of the central individual with his personal exterior on the top right, his personal interior on the top left, the interior of the groups to which he belongs on the bottom left, and the interior of these groups on the bottom right. In other words, the individual’s measurable and visible aspects are in the upper-right quadrant, those of the groups to which he belongs in the lower-right quadrant. The aspects that the individual experiences are in the upper left quadrant, while phenomena that arise and are shared collectively belong in the lower left quadrant.
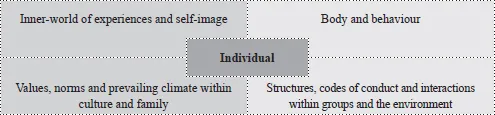
More concretely, the top right-hand corner is the quadrant of biological, physical properties and all aspects of behaviour (for these are quantifiable aspects). Top left is the quadrant of the personal world of experience of thoughts, feelings, emotions, intentions and self-image, while the bottom-left quadrant stands for values, norms and beliefs within family and culture, including psychological system dynamics and group processing. Finally, the lower right corner of the quadrant houses the socio-economic context, including characteristic features, rituals, regulations and environment. For clinical practice, we remember the following keywords: ‘body and behaviour’ (top right), ‘inner-world of experiences and self-image’ (top left), ‘values, norms and prevailing climate within culture, group and family’ (bottom left) and ‘structures, codes of conduct and interactions within groups and the environment’ (bottom right) (Figure 1.2).
Figure 1.1The Four Quadrant Model
Source: Based on Wilber, 1998b, 2000, 2001a, 2006, 2017
Figure 1.2The Four Quadrant Model
Source: Based on Wilber, 1998b, 2000, 2001a, 2006, 2017
At the same time, Wilber points out that the 4QM can be seen as two halves that represent a specific scientific view of the world. The two quadrants on the right, can be approached with an empirical-analytical perspective and obey the ‘measuring is knowing’ rule, while the entire left can be accessed via a phenomenological-hermeneutical and dialectical approach in which interpretation and meaning are central (Figure 1.3). We recognise these two scientific perspectives as the characteristic paradigms of the spectrum of therapies that we outlined in the introduction. The 4QM, therefore, consists of a subjective left half and an objective right half.
A direct and clinical consequence of this for the therapist is the need to consider both sides if the patient is to be portrayed as fully as possible. In concrete terms, this means that the therapist does not merely zoom in on a child’s problematic behaviour, for example, as is the case within the DSM culture, but that he tries to understand the meaning layer underlying this ‘behaviour as a phenomenon’.5 This is exactly why the ICF model misses the mark for the first time. After all, the ICF model is mainly concerned with the individual’s external, measuring and visible factors and his or her participation in society. In the 4QM, this corresponds to the top-right quadrant and the bottom-right quadrant, respectively. In a certain sense, therefore, the ICF model focuses on only two of the four quadrants, i.e. one half of human reality, i.e. only the part that can be charted empirically. As said before, the 4QM tries to show human reality in a more inclusive way.
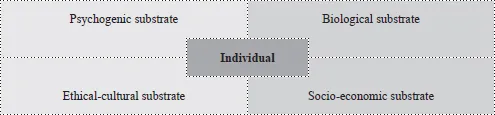
The 4QM, therefore, relates to several substrates that hide behind the condition humaine. Translated to professional healthcare, we can discover four of them (Figure 1.4). The biomedical substrate in the top right belongs to doctors, physiotherapists, manual therapists and osteopaths. The psychological substrate of the top left quadrant belongs to the domain of clinical psychologists and psychotherapists, while the ethical, systemic and cultural-philosophical substrate in the bottom-left corner is more specifically the work domain of couples and system therapists, philosophical counsellors and ethical experts. Finally, the bottom-right quadrant is based on a socio-economic substrate where, in terms of professional healthcare, we can situate institutions such as public social welfare centres or employment agencies. Here, social workers are involved in debt mediation, support for problematic parenting situations or guidance in employment or training.
Figure 1.3The Four Quadrant Model and paradigms
Source: Based on Wilber, 1998b, 2000, 2001a, 2006, and 2017
Figure 1.4The Four Quadrant Model
Source: Based on Wilber, 1998b, 2000, 2001a, 2006, and 2017
Although we must not lose sight of the fact that the 4QM as a didactic model is only intended as a coat hanger for inventory and differentiation, its strength also lies in its integration on the basis of the following basic principles:
each individual can be situated within the 4QM
and consists of at least 4 domains of expression, housed in four quadrants
these are not reducible to each other
each speak their own language
each have their own entry point to reality
are intrinsically intertwined
and therefore, cannot be separated from each other’s dynamics and influence.
Translated to patients, this means that we, as care providers, must ensure that the complex reality in which our patients find themselves is not reduced to less than four quadrants. In concrete terms, this happens when, for example, depression is reduced to a mere – usually hereditary – issue of a disrupted metabolism of serotonin and dopamine, without valuing experiences, thoughts and self-image as being at least as important and influential. In other words, depressive feelings and thoughts are not simply the result of a disturbed neurotransmission, but are a unique partial reality in themselves. In quadrant terms, the top left quadrant is not an epiphenomenon of the top-right quadrant, but equally a unique expression of the individual.6 Subsequently, as a care provider, we must make sure that a balanced approach, such as 4QM, does not blind us to what is ‘normal’ in our patient’s story. For example, when Horwitz and Wakefield (2007) suggest in their book, The loss of sadness, that we have all relegated normal sadness to an area referred to as clinical depression, they point to the DSM as the decisive factor. Distinguish at least four domains in which the reality of the patient expresses itself and be vigilant when labelling a patient as being ‘abnormal’ or ‘pathological’ too quickly. In addition to precise differentiation – for example, during the anamnesis – 4QM then also helps to select the right language or entry point to approach the patient.7 What does the patient currently need most, what can he handle and what appears to be the most helpful? Around which possible entry points – talking, moving or touching for example – is there resistance or anxiety? What about self-reliance and can the patient rely on a stable support network if necessary, or is guidance needed at this level? We will return to this in mor...
Table of contents
Cover
Half Title
Title
Copyright
Dedication
Contents
List of figures
Foreword
When reading this book
Some opening reflections
Some testimonials
Introduction: The psychosomatic body in a field of therapies
1 An integrated look at the psychosomatic patient
2 The narrative patient
3 The body in therapy: possible or not?
4 The tense body
5 The unconscious within experiential bodywork
6 The psychosomatic body within the fulcrum model
7 The practice of experiential bodywork
In retrospect
Bibliography
Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
Both plans are available with monthly, semester, or annual billing cycles.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go. Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Treating Psychosomatic Patients by Joeri Calsius in PDF and/or ePUB format, as well as other popular books in Psychology & Mental Health in Psychology. We have over 1.5 million books available in our catalogue for you to explore.