Health care is increasingly under pressure. Budget crises are making collaboration and smart thinking essential, while increasing numbers of people with multiple long-term conditions make specialist models of health care increasingly inefficient – patients too often go from one specialist to another, duplicating effort and paying too little attention to the bigger picture of their health.
Collaborating for Health outlines a solution: community-oriented integrated care and health promotion. Designed to prevent the problems of fragmented care, this approach focuses on building teams, networks and communities for health and care at local level, where it is easier to see the range of factors that affect people's health. With the emphasis on partnership-working between primary care, public health and others, it allows clusters of general practices to share the work of integrating efforts for care and health improvement, and for non-medical organisations to lead parallel initiatives for health and care. Introducing both horizontal and vertical integration, Thomas presents ways to develop community-oriented integrated care in a sustainable way, and how to practise the skills in small ways before you have to perform on a big stage.
This guide is for anyone interested in how multidisciplinary primary care teams can orchestrate most aspects of health and care at local level, with timely specialist input.
Image to support Part I: Connected learning spaces
Introduction to Part I: Community-oriented integrated care depends on trusted relationships
Box: Policy that supports community-oriented integrated care
Chapter 1: Communities for health. Localities of 30–70,000 population – health networks and local health communities – are a good ‘village’ size to build relationships between extended primary care teams that help everyone to integrate their ways of working.
Chapter 2: Shared care for long-term conditions. Most medical care for long-term conditions such as diabetes should happen in general practices (tier one). Tier two is a community-based clinic that supports tier one and aligns specialist teams to localities. Tier three is hospital care. Summaries of patient-held care plans are available to those who make ad hoc contributions.
Chapter 3: Seasons of learning and change. People from different parts of health care naturally do similar things between January and March, April and July, September and October, and November and December. These four ‘seasons’ help to build a calendar of events for shared care, health promotion and participatory action research. Routinely gathered data help to evaluate the overall effect.
Chapter 4: Infrastructure of facilitation and communication.Applied research units evaluate and maintain infrastructure to support annual cycles of inter-organisational reflection and collaborative improvement. They establish leadership teams, strategic partners, live manuals, stakeholder workshops, data gathering, publications and learning between case study sites.
Who might find Part I useful?
This part is primarily for policymakers, although others may also find it useful. It describes infrastructure to build and sustain local communities for health, and systems for shared care. These are needed to build community-based coordinating hubs that will help to realise the WHO concept of comprehensive primary health care – whole-society collaboration for whole population health. It also makes primary care more efficient.
This book advocates a participatory and systematic way to improve services that usually happens in more top-down and ad hoc ways. An annual calendar of events stimulates inter-organisational learning and change within and between local health communities – geographic areas of about 50,000 population. Clusters of general practices in these areas develop extended primary care teams and contribute to leadership of local initiatives in partnership with policymakers, public health, specialist services and many others.
Different local health communities pilot different things, led by local multidisciplinary shared leadership teams. An applied research unit supports them to lead the processes, evaluate outcomes and share learning. Seasons when everyone does similar things at the same time shape an annual calendar of linked events for cycles of inter-organisational learning and change. This fosters a development approach that is participatory and evolutionary. It enables local discussions that link local concerns with bigger pictures.
The approach considers people to be connected as though they are cells in the ‘body’ of health care, as well as components in a machine. If we want people from different parts of a system to integrate their efforts for care and health promotion we need more than mechanical linkage. Integration also requires us to build trusted relationships across disciplinary and organisational boundaries. ‘Vertical’ care pathways are not enough. We need ‘horizontal’ team-working between people of different insights too.
‘Horizontal’ team-working is needed for many purposes – patient care plans, co-design of services and health promotion campaigns, for example. Team-working is easier to achieve when people are aligned to the same geographic area – it is easier for everyone to get to know the others and align the plans of their organisations. In time, networks of relationships can become interwoven to create a sense of a local community – large numbers of people feel ‘on the same side’ ready to reinforce health messages, provide mutual support and collaborate for improvement projects. The best size of the area depends on the local situation. In UK cities, 50,000 is a good ‘village’ size – small enough to feel you belong and large enough to have political impact. But you have to consider your specific situation.
Geographic areas provide the opportunities for other organisations to lead initiatives in the same area that complement the effect of others; for example schools, faith groups, social services, voluntary groups. Merely acknowledging that they are contributing to a broader quest for whole-society health helps everyone to feel united. Each year different things happen depending on what different individuals and groups can manage.
Shared care, care plans and improvement projects emerge from this activity and provide opportunities for participants to develop their skills as team players. Shared leadership teams can improve their skills through learning sets and leadership courses. Networks of such teams can link with policy-making processes to make top-down and bottom-up initiatives enhance each other.
This part shows how to systematically develop and sustain infrastructure for integrated working at local level. Policy can chart a course to achieve this even in turbulent times. Keep your eyes focused on practical ways to apply the principles in your situation.
Image to support Part I: Connected learning spaces
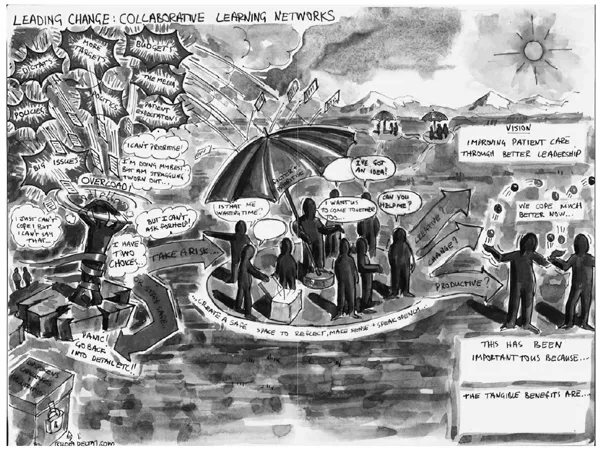
This picture was drawn by Julian Burton (Delta7 Change Ltd – www.delta7.com) to portray the shared vision of a west London CCG.
Uncertainty is inevitable when improving health and integrating care, because everything is constantly changing in response to changes elsewhere. Unfortunately, uncertainty leads to anxiety in some people, causing them to disengage, obstruct or micro-control – behaviours that lead to poor outcomes.
Success comes from engaging with this complexity and acting at the right times to make progress that is, and feels, positive.
Trusting, learning spaces (the umbrellas) reduce anxiety by clarifying plans and sharing risk. They are more than places to coordinate activities. They include work-shops where stakeholders critique plans and consider new developments. Facilitators help participants to learn from and with each other as they solve problems, share insights and generate improvement projects. The trust that is generated makes it possible to say things that might be considered ‘undiscussable’ – the ‘elephants in the room’.
These workshops can be linked, so learning in one place can be considered in others. Events can be strategically linked to support annual cycles of collaborative learning and coordinated change that help local health communities to develop. Even more – different cycles of learning can link across much larger areas to enhance learning and influence, and create a culture of continual quality improvement. Scheduling workshops well in advance helps people to engage at appropriate times.
Figure I Connected learning spaces
Introduction to Part I: community-oriented integrated care and health promotion depends on trusted relationships
Community-oriented integrated care (COIC) is shared care and collaborative health promotion at local, community level. At local level it is easier to see the large number of factors that affect someone’s health. Further away, for example in hospital, conversations tend to focus on the reason for being there – usually an illness.
The secret ingredient of integrated care is a trusted relationship. You can get things done when the people you relate to (patients, professionals, neighbours, friends) react positively to you. Trust means that others will adapt their work to support yours, do the things they said they would, signpost resources you don’t know about, give constructive criticism, and make honest assessments about whether they can add anything useful. Trusted relationships make people feel on the same side and more...
Table of contents
Cover
Half Title
Title Page
Copyright Page
Dedication
Table of Contents
About the author
Acknowledgements
Forewords
Endorsements
Who is the book for?
Bring your own case study
Introduction
Part I Policy to support integrated working
Part II Integrating care and promoting health from local organisations
Part III Integrating care and promoting health from geographic localities
Part IV Understanding community-oriented integrated care
Part V Community-oriented integrated care – making it work
Appendix: Skills to lead community-oriented integrated care
Bibliography
Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.4M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
Both plans are available with monthly, semester, or annual billing cycles.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go. Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Collaborating for Health by Paul Thomas in PDF and/or ePUB format, as well as other popular books in Medicine & Public Health, Administration & Care. We have over one million books available in our catalogue for you to explore.