![]()
1
What Do We Mean by Specialist Hospital, Intensive Community and Home-Based Services?
Tim McDougall
Key points
- One of the most important landmarks in the history of CAMHS strategy in the UK was the 1995 NHS Health Advisory Service’s ‘tiered model’ of service delivery. Nearly 20 years since its inception the tiered model remains the preferred framework to organise the commissioning, management and delivery of mental health services for children and young people with mental health problems and disorders in the UK.
- The evidence base for Tier 4 CAMHS is in its infancy. Evidence for some services is poorly developed, and for others it is based on US or European services where systems for commissioning and providing healthcare are different to those in the UK.
- The predominant model of intervention in Tier 4 CAMHS for young people in the UK remains admission to hospital. The models of care that exist as alternatives to admission are intensive community and day care, intensive outpatient treatment and home-based services. However, these are not routinely available across the UK and in some areas are few and far between or not available at all.
- The effectiveness of hospital, intensive community and home-based services depends on a number of essential factors. These include early intervention, a thorough knowledge of the child or young person, interventions that focus on difficulties and problems across multiple domains of functioning, adherence to treatment and completion of the therapeutic programme.
- The delivery of effective interventions for children requiring hospital, intensive community and home-based services depends crucially on an appropriately trained, skilled and experienced workforce. Working with children and young people with complex psychosocial needs can be a challenging and emotionally draining process. It is therefore important that those providing care and treatment interventions have access to supervision and support from skilled practitioners
Introduction
This chapter discusses what we mean by hospital, intensive community and home-based services in the UK policy and planning context. Definitions offered by clinicians and commissioners are compared. The evidence base for the range of services that are broadly referred to as Tier 4 is summarised, and good practice distilled from what is known about the success of existing services is discussed.
Background
The most important strategic document to set the context in which CAMHS in the UK have evolved was the NHS Health Advisory Service (HAS) report, Together we Stand (NHS Health Advisory Service 1995). This provided a detailed summary of the characteristics of nationwide CAMHS, with chapters on epidemiology, needs assessment, service principles, and the commissioning and provision of services. The report led to widespread use of the acronym ‘CAMHS’ and applied the four tiered framework to help promote the important message that child and adolescent mental health is everyone’s business. In this report Tier 4 CAMHS were described as follows:
Tier 4 provides for highly specific and complex problems which require considerable resources. These include, for example, inpatient psychiatric provision for adolescents, secure provision, specialist facilities for those with sensory handicaps, very specialised services (outpatient and inpatient) for young people with severe eating disorders, specialised neuropsychiatric out-day and inpatient services and consultation services for rare paediatric disorders.
(NHS Health Advisory Service 1995)
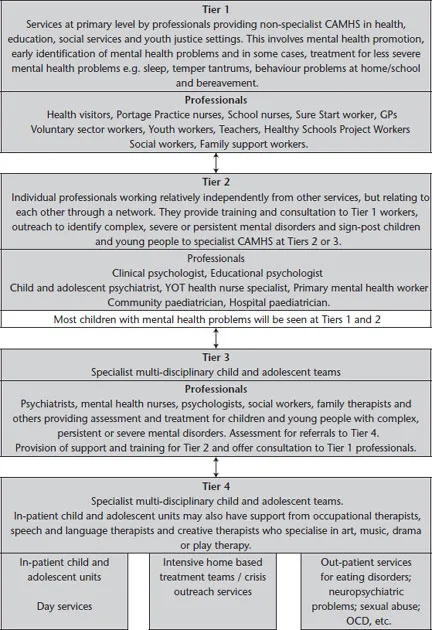
Whilst it has not been without criticism the ‘tiered model’ of service delivery remains the preferred framework to organise the commissioning, management and delivery of mental health services for children and young people with mental health problems and disorders in the UK. The ways in which the tiered model operates, both by design and by accident, are discussed further in Chapter 2 which focuses on the clinical pathways to hospital, intensive community and home-based services. However, for the purpose of setting the context for this chapter and the book which follows, it is outlined in Figure 1.1.
Figure 1.1 NHS Health Advisory tiered model of service delivery (1995) (Source: McDougall, 2006)
Tier 1
Parents and professionals in primary, universal or front-line services are usually the first to recognise that children and young people may be struggling. These include general practitioners (GPs), teachers, school nurses and health visitors. Tier 1 services are those in which children and young people receive day-to-day healthcare or education. They are provided in GP practices, schools and social care settings, and workers in these settings should have a basic understanding about self-harm and know how to refer a child for primary care or more specialist assessment.
Tier 2
Tier 2 services are provided by professionals with additional training or expertise in child and adolescent mental health. Their role is to provide direct assessment or treatment for individual children and young people with less complex problems than those requiring most specialist interventions at Tier 3 or 4 services. They also provide support, guidance and training for Tier 1 professionals providing front-line services.
Tier 3
Professionals working in services at Tiers 1 and 2 must be able to access specialist CAMHS where they have concerns about the mental health of a child or young person they are working with. Tier 3 services are dedicated multidisciplinary teams providing comprehensive assessment, treatment and consultation services for children and young people with complex, persistent or severe mental health needs and disorders. Tier 3 teams usually comprise psychiatrists, psychologists, nurses, family therapists, social workers and other therapists. They offer a range of psychological and pharmacological treatments.
Tier 4
Tier 4 services are highly specialised tertiary CAMHS and include inpatient child and adolescent units, specialised eating disorders services and forensic CAMHS, as well as multi-agency services such as home treatment services, community support teams and crisis teams. It is these services which are described in detail throughout this book. The Royal College of Psychiatrists (2006) also refer to ‘non NHS Tier 4 settings’ including specialist residential schools and social care homes, specialist foster care, enhanced social services residential placements and local authority secure units. The College suggests that such settings may or may not have mental health as a focus of their work and may or may not have specialist mental health workers in their teams.
Policy definitions
A significant landmark in the development of Tier 4 services was the National Service Framework (NSF) for Children, Young People and Maternity Services (Department of Health 2004). In this framework for commissioning and providing children’s services, Tier 4 CAMHS were defined as follows:
Highly specialised comprising intensive outpatient services; assertive outreach teams; inpatient residential and secure provision; and other highly specialised assessment, consultation and intervention services. Amongst the highly specialist services, inpatient psychiatric units for both children and adolescents, but separately provided to ensure that the developmental needs of different age ranges are met, are essential resources, representing ‘the intensive care of child mental health’. A network of care is required in each locality for children and young people with severe, challenging and complex problems. This will promote collaborative working between services such as therapeutic fostering, pupil referral units, secure units, adolescent in-patient units and children’s homes. Tier 3 and Tier 4 have a role in providing mental health services to secure units (e.g. secure children’s homes, secure training centres and young offenders institutions), residential education and residential care, together with other intensive community settings, e.g. specialist fostering.
To achieve this vision for Tier 4 services the Department of Health made a number of policy declarations and set standards for service providers and commissioners. Multi-agency and specialist commissioning and planning were to drive and shape Tier 4 services according to need and best practice, enabling the delivery of a volume of services that would encompass the challenges of demand, capacity, diversity and capability. Emergency care, general and specialist inpatient services (e.g. eating disorders, forensic, medium secure and learning disability) would be available for children and young people from each locality. The numbers of beds was to be matched to need for each locality. Patients who should be admitted on clinical grounds would not be refused access due to limitation of resources such as bed availability.
Primary Care Trusts (PCTs) and local authorities were to ensure that a network of care was developed in partnership for the provision of Tier 4 services, and that written criteria for admission were to be available and understood by professionals working with children and young people. Health providers of Tier 4 CAMHS were expected work in collaboration with specialist education, social care and youth justice provision to provide a network of services for children and young people with severe, challenging and complex problems. Furthermore, PCTs and local authorities were to ensure that local networks of care were developed between Tier 3 and Tier 4 services to include assertive outreach and day care as well as inpatient and community services. Specialist CAMHS were to become involved in the provision of mental health services to secure units, residential education and residential care, together with other intensive community settings such as within specialist fostering. There was to be close collaboration and liaison with adult mental health services.
The NSF stated that there needed to be a shared understanding of the level of care required on discharge from inpatient services and the appropriate resources available across community services. Shared aftercare arrangements and transition protocols between CAMHS and general adult psychiatric services were to be agreed and subject to audit. When children and young people were unavoidably placed on paediatric or adult psychiatric wards, there was to be collaboration and joint working between child health, adult mental health and CAMHS professionals.
To help map progress against standard 9 of the NSF the University of Durham led a CAMHS mapping project which gave more detail to an expanded definition of ‘Tier 4 Special Care Teams’. Special care included the provision of treatment or care more often than weekly or twice weekly through inpatient care, outreach support and intensive aftercare. Day services and intensive fostering also fell into this category, as did intensive home visiting and/or frequent and unscheduled attendance at day care to avert the need for residential care.
The new ‘post-NSF’ world
Nearly a decade on, the NSF may soon be replaced by a new strategy, and it is disappointing that the range of services and the underpinning standards that were in the framework have still not been developed in some parts of the UK.
Nearly two decades following the introduction of the tiered model in CAMHS, responsibility for commissioning Tier 4 services across England has transferred from local clinical commissioning groups to NHS England. The clinical reference group that has been advising the Department of Health on what Tier 4 services should comprise have developed the specifications that will inform commissioning, and ultimately service provision.
The ...