Assisted Reproduction is a specialty undergoing rapid change as new technologies are introduced and new research challenges previous treatment options. This text examines a selection of controversial topics for both laboratory and clinical practice and tries to place them in perspective, so readers can understand how and why the current state of the question has come about and how future contributions to the debate should be measured. All physicians involved with the technologies concerned will learn from the expert contributions assembled here.
CONTENTS: The use of ovarian markers * Use of molecular markers of endometrial receptivity * Use of GnRHa for triggering final oocyte maturation during ovarian stimulation cycles * Use of time-lapse embryo imaging in assisted reproductive technology practice * Use of cryopreservation for all embryos * Preimplantation genetic screening * The use of single embryo transfer * Use of luteal phase support * Measuring safety and efficiency in in vitro fertilization * To flush follicles during egg collection or not * Use of blastocyst culture * Use of mitochondrial donation * Controversies in recurrent implantation failure: From theory to practice * Fibroids: To remove or not? * Limitations of endometrioma surgery in in vitro fertilization: Possibilities of early disease control

eBook - ePub
Controversies in Assisted Reproduction
- 144 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
Controversies in Assisted Reproduction
About this book
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
Topic
Medicine1
The Use of Ovarian Markers
Neena Malhotra and Siladitya Bhattacharya
Introduction
Ovarian reserve is a term used to describe a woman’s reproductive potential and is a reflection of her pool of primordial follicles or, more specifically, the number and quality of oocytes in her ovaries (1). Each woman is born with approximately 2 million primordial follicles, but this number drops to 400,000 around menarche as a consequence of follicular atresia (2). Follicle numbers fall further with age, and the rate of decline is faster when women are in their mid-30s. This decline in fertility potential is specific for an individual woman and is influenced by race as well as genetic and environmental factors.
The ideal ovarian reserve test should be convenient, reproducible, display little if any intracycle and intercycle variability, and demonstrate high specificity to minimize the risk of false diagnoses. At the same time, the test should be able to identify women with an abundance of ovarian reserve and those who are likely to respond vigorously to ovarian stimulation in the context of fertility treatment. A number of biomarkers have been used over the last few decades to predict ovarian response and pregnancy outcomes, including live birth in women undergoing in vitro fertilization (IVF). These include hormonal assessments and ultrasound parameters.
Hormonal biomarkers include serum early follicular (basal) levels of follicle-stimulating hormone (FSH), estradiol (E2), inhibin B, and anti-Müllerian hormone (AMH), as well as dynamic tests that measure gonadotropins and estradiol levels in response to stimulation, like the clomiphene citrate challenge test (CCCT), GnRH-agonist stimulation test (GAST), or exogenous FSH ovarian reserve test (EFORT).
Ultrasonographic assessments include antral follicle count (AFC) and ovarian volume. The number of antral follicles reflects the size of the remaining follicular pool and correlates with the number of oocytes retrieved following stimulation. Ovarian volume declines with advancing age and is a potential indicator of ovarian reserve.
This chapter considers the basic principles governing the use of diagnostic tests and reviews common tests of ovarian reserve including their role in predicting fertility with and without assisted reproduction treatment.
Understanding Diagnostic Tests
As diagnostic tests are seldom 100% accurate, tests need to be validated by comparing them with an ideal test or a gold standard in a suitable population of patients. A valid test is able to identify most people with a particular condition and exclude most people without that condition such that a positive test result means that the disorder in question is present (3). Conventionally, four terms are used to qualify the validity of a test—sensitivity, specificity, positive predictive value, and negative predictive value (Figure 1.1). Sensitivity is the true positive rate that expresses how good the test is for correctly identifying those with the condition. In contrast, specificity is the true negative rate that tells us how good a test is for correctly excluding people without the condition.
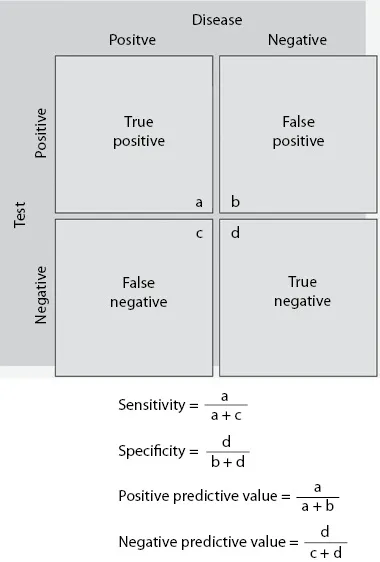
Figure 1.1 Calculation of test validity. (With permission from Grimes D, Schulz K. Lancet. 2002;359[9309]:881–4.)
As both sensitivity and specificity represent a retrospective analysis of results that have already been collected, their clinical use is limited. In real life, clinicians need to know the predictive value of the test, i.e., whether a patient who tests positive actually has the disease or condition in question. Positive predictive value is the posttest probability of a positive test. It tells the clinician what the probability of having that condition is if the patient tests positive. Negative predictive value tells the clinician the probability of a patient not having a condition if the patient tests negative. It is customary to express the validity of the test by plotting sensitivity against one minus specificity and measure the area under the curve (AUC). AUC is an effective way to summarize the overall diagnostic accuracy of the test by plotting values between 0 and 1 (Figure 1.2), where a value of 0 indicates a totally inaccurate test and a value of 1 a perfectly accurate test. An AUC of 0.5 indicates an inability to diagnose patients with and without a particular condition, while 0.8–1.0 is considered excellent (6).
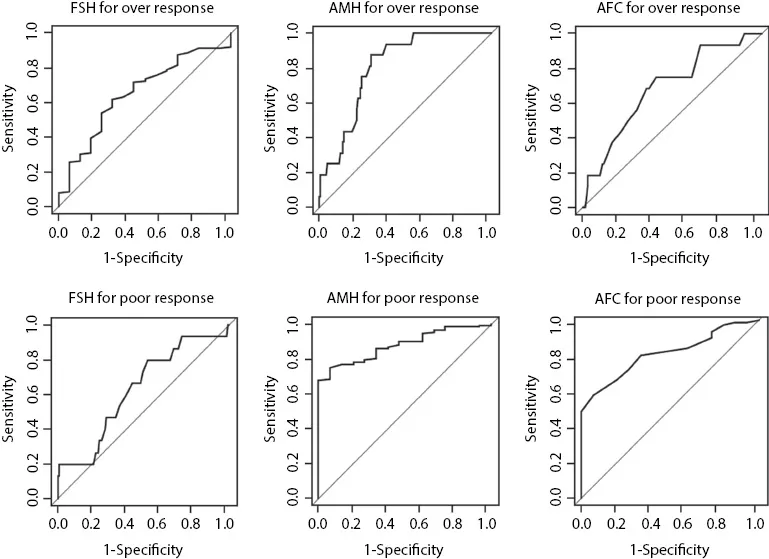
Figure 1.2 Receiver operating characteristic curves and area under the curve for a number of common ovarian reserve tests. (With permission from Nardo L et al. Fertil Steril. 2009;92[5]:1586–93.)
The prevalence of disease in a population affects the performance of screening tests. Even excellent tests have poor predictive value positives in low-prevalence settings. For example, a valid test of ovarian reserve will have a better positive predictive value in women attending a fertility clinic than in a general population of asymptomatic women. Hence, knowledge of the approximate prevalence of disease is a prerequisite to interpreting screening test results. Inappropriate application or interpretation of screening tests can rob people of their perceived health, initiate harmful diagnostic testing, and squander health-care resources. From a clinical perspective, key questions about tests include the following: Is it relevant, i.e., can the test be used in the relevant patient group? Is it affordable, acceptable, and better than the test normally used? And crucially, Will it inform the choice of treatment?
Early Follicular Follicle-Stimulating Hormone
Levels of basal FSH in the early follicular phase have been used as a biomarker for the prediction of response to ovarian stimulation during in vitro fertilization (IVF) (7,8). The test is based on the feedback inhibition of FSH pituitary secretion by ovarian hormones. Women with normal ovarian activity should produce sufficient levels of ovarian hormones at this early stage of the menstrual cycle to suppress FSH levels within a normal range. Elevated serum FSH levels suggest poor production of ovarian estrogen by a smaller follicular pool consistent with diminished ovarian reserve (DOR). However, basal FSH testing has several major limitations, including significant intercycle and intracycle variability (9,10) and limited sensitivity when used in isolation. Measurement of both FSH and estradiol on cycle day 3 may therefore help decrease the incidence of false-negative testing. Despite its limitations, FSH is commonly used as an ovarian reserve test, and high values have been associated with both poor ovarian response and failure to achieve pregnancy (11). FSH has relatively high specificity (45%–100%) for poor response to ovarian stimulation (usually defined as less than four retrieved oocytes) using cutoff points beyond 10 IU/L (10–20 IU/L), but its sensitivity is generally poor (11%–86%) (11,12). In terms of predicting lack of conception, FSH testing is still specific (50%–100%) but much less sensitive (3%–65%) using similar cutoffs (11,12). This test is still clinically useful since an abnormally ele...
Table of contents
- Cover
- Half Title
- Dedication
- Title Page
- Copyright Page
- Contents
- Contributors
- 1. The Use of Ovarian Markers
- 2. Use of Molecular Markers of Endometrial Receptivity
- 3. Use of GnRHa for Triggering Final Oocyte Maturation during Ovarian Stimulation Cycles
- 4. Use of Time-Lapse Embryo Imaging in Assisted Reproductive Technology Practice
- 5. Use of Cryopreservation for All Embryos
- 6. Preimplantation Genetic Screening
- 7. The Use of Single Embryo Transfer
- 8. Use of Luteal Phase Support
- 9. Measuring Safety and Efficiency in In Vitro Fertilization
- 10. To Flush Follicles during Egg Collection or Not
- 11. Use of Blastocyst Culture
- 12. Use of Mitochondrial Donation
- 13. Controversies in Recurrent Implantation Failure: From Theory to Practice
- 14. Fibroids: To Remove or Not
- 15. Limitations of Endometrioma Surgery in In Vitro Fertilization: Possibilities of Early Disease Control
- Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Controversies in Assisted Reproduction by Botros Rizk, Yakoub Khalaf, Botros Rizk,Yakoub Khalaf in PDF and/or ePUB format, as well as other popular books in Medicine & Gynecology, Obstetrics & Midwifery. We have over 1.5 million books available in our catalogue for you to explore.