eBook - ePub
Spatial Neglect
A Clinical Handbook for Diagnosis and Treatment
- 161 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
Spatial Neglect
A Clinical Handbook for Diagnosis and Treatment
About this book
Spatial neglect is a profound clinical problem as well as intriguing scientific problem. In the last ten years, there has been an explosion of interest in this disorder, which as a result is no longer viewed as a single entity, but rather as a number of different disorders. This book is an attempt to bring the reader up to date with the latest advances in understanding neglect, at least insofar as this contributes to better clinical assessment, management and treatment. This is not a book for the specialist researcher in the neuropsychology of neglect and attention. Rather, it is a book aimed at clinicians - student and trained - from all disciplines involved in the assessment, management and treatment of neglect.
The book begins with the description of four cases manifesting different types of unilateral neglect. The reader is introduced to different aspects of neglect through these patients. These distinctions include those between personal and extrapersonal neglect, motor versus sensory neglect and many others. The reader is also introduced to other phenomena that are closely related to neglect, including ansognosia and impaired sustained attention. The latest methodes of assessment of neglect are also described, as are methods of treatment, again with reference to the four introductory specimen cases.
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
CHAPTER ONE
Clinical presentation of spatial neglect
INTRODUCTION
Many patients who survive brain damage are left with a variety of cognitive difficulties which can adversely affect their recovery and treatment. The term “cognitive” is used here to describe a wide range of mental abilities including perception, reasoning, memory, and language. Cognitive impairments are often missed or poorly described in clinical practice, yet they often influence the patient’s recovery and may explain the patient’s failure to respond adequately to rehabilitation. As many types of everyday cognitive activities involve directing attention to selective spatial features of our environment, it is not surprising that visuospatial disorders after brain damage are sometimes difficult to identify or characterise.
Adequate visual perception and spatial perception is necessary, however, for most daily activities, e.g. dressing, object manipulation, drawing, finding one’s way about, reading, walking and acquiring new motor skills. The importance of visuospatial disturbances has tended to be underestimated, involving as they do the location of the person with respect to the world and its objects, and the relation of these objects to each other. These disorders, which are commonly encountered after right hemisphere stroke, have been shown to constitute a substantial impairment for functional recovery. Furthermore, they can limit the effectiveness of rehabilitation, often to a greater extent than more obvious motor, sensory, and speech deficits (Halligan & Cockburn, 1993). Evidence from several stroke studies indicates that the most disruptive and common visuospatial symptom after right-sided stroke remains unilateral (visual) neglect—the focus of this book.
Although unilateral visual neglect, or hemi-inattention, represents one of the most common visuospatial disorders, it still remains poorly understood. In this book, we focus on the clinical assessment and rehabilitation of visual neglect. Although the book will provide a general overview of current research findings, the intention is not to replicate recent specialised texts concerned with the theoretical mechanisms thought to explain the condition. For a comprehensive review of the neuropsychology of neglect, the interested reader is directed to Bradshaw and Mattingley (1996); Halligan and Marshall (1994d); Heilman, Watson, and Valenstein (1993); McCarthy and Warrington (1990); Robertson and Marshall (1993); Jeannerod (1987); and Weinstein and Friedland (1977b).
WHAT IS NEGLECT?
Unilateral neglect or hemi-inattention are clinical terms used by neurologists, neuropsychologists, and therapists to describe a family of often different behavioural symptoms characterised by the patient’s failure to attend or respond to objects or people in selective parts of space. The term “neglect” has often been used imprecisely to cover a host of sensory, perceptual, and attentional deficits. When used to describe the clinical condition that typically follows right brain damage, the term describes the failure to report, respond, or orient to novel or meaningful stimuli—usually, but not always, on the side of space or objects opposite the side of the lesion. The term “neglect” cannot be meaningfully used if the target behaviours can be explained by either primary sensory or motor deficits (Heilman et al., 1993). Within clinical practice, unilateral neglect was initially considered to be a single syndrome (Heilman et al., 1993). However, the set of behaviours attributed to this syndrome suggests that it is unlikely to be a unitary disorder and many different types of neglect have now been described (Halligan & Marshall, 1994d).
Neglect failed to receive serious theoretical and clinical interest until the late 1970s, due in part to the implicit assumption that it could somehow be explained by the patient’s failure to compensate for more obvious sensory and motor problems. Neglect, however, is more than a visual field cut, hearing loss, or motor weakness. Many “neglect behaviours” cannot be adequately explained in terms of sensory or motor loss. Although many patients do indeed have visual field deficits and hemiplegia, severe neglect can be seen in patients without such deficits. Furthermore, the lesions that produce visual neglect are not necessarily limited to the primary sensory or motor areas of the brain.
As many patients with neglect believe that they have an adequate perception of the world, the necessity to make adjustments such as turning their heads to look and search for missing objects on the affected side is not obvious. Consequently such patients often present with additional problems of minimisation, rationalisation, denial, and/or confusion.
In the absence of adequate primary sensory or motor explanations, a variety of neuropsychological accounts have been put forward to explain the condition; most of these characterise the condition as a set of attentional disorders, although other explanations emphasise perceptual, representational, intentional, and pre-motor factors. These accounts no longer consider explanations in terms of a disorder of seeing, hearing, feeling or moving but rather one that involves a disturbance of looking, listening, touching, and exploring space (Mesulam, 1981).
CLINICAL DESCRIPTIONS
Throughout the book, the typical illustrations of left neglect after right brain damage (RBD) are adopted. Patients with neglect often collide with objects on their left side, fail to eat from the left side of the plate, and dress only one side of the body. Illustrations of this striking behaviour in the case of drawing are shown in this chapter. Clinically, visual neglect is often associated in the acute phase with a marked deviation of the head, eyes, and trunk towards the side of lesion. In more serious cases, patients fail to recognise their contralateral extremities as their own, and only attend to those events and people situated on the ipsilesional side. Neglect may encompass several sensory modalities and involve aspects of personal, extrapersonal, and representational space. Many patients, not surprisingly, show difficulties in reading, written arithmetic, writing, and drawing as a result.
For many patients, visual neglect is not a transitory problem. A study by Kinsella and Ford (1985) showed that the effects of visual neglect can persist up to 18 months post stroke. Features of neglect can continue to be insidiously disruptive in many areas of the patient’s daily life long after the resolution of florid symptoms. Zarit and Kahn (1974) reported features of neglect up to 12 years post stroke. The persistence of visual neglect has significant ramifications, as stroke patients comprise a large proportion of those treated in hospital and rehabilitation centres. Many of these patients require close supervision in daily activities, as they are particularly prone to accidents. Visual neglect limits, therefore, the degree of active participation in retraining programs and is commonly associated with poor functional recovery.
To provide the reader with a clinical picture of the complex presentation of neglect, we present four cases that help illustrate the range of neglect phenomena commonly seen after right brain damage.
Case 1: John
Clinical presentation. John is a right-handed businessman who suffered a stroke that affected movement on the left side of his body. Before his stroke, John suffered from angina and had been treated for hypertension. John’s stroke paralysed his left leg and arm and cut off vision on the left side. John now complains that he cannot see the nurses or doctors when they talk to him on his left side. A CT scan (Fig. 1.1) showed a large area of damage located on the right side of his brain. Over the next four weeks, John’s arm and leg began to improve slowly; however, nursing staff at the hospital noticed that John’s most disabling problem was his apparent unawareness of people and objects located on his left side.
Behavioural observations. On the ward, John could be seen searching for his spectacles which were in fact located on the left side of the table in front of him. His hand feels along the surface of the tabletop but never quite makes the last 6 inches (on his left) which separates him from his glasses. Despite several head turns to the left, his eyes appear to scan only those objects located on the right side of the table. When the nurse approaches from his left and asks John if he has filled out his menu card for the week’s meals, he initially fails to respond to her, even though his hearing is otherwise normal. When the nurse calls his name loudly several times, he does eventually, but slowly, move his eyes and head round in small jerky movements and replies to her. When requested to look further to his left, John eventually finds his glasses; while picking them up, he notices the menu card which had been lying immediately to the left of them. He reads from the menu card but as the days’ choices are lined up from the left side of the card, John checks only those items from Friday through Sunday, leaving Monday to Thursday blank. Finally, when his food does arrive he also misses the potato on the left side of his plate (see Fig. 1.2 for a typical illustration).
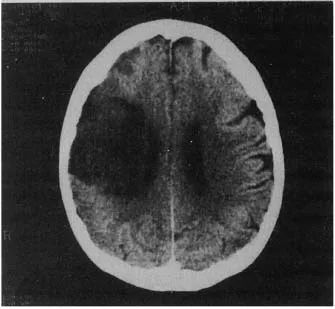
FIG. 1.1 CT scan (right on left) of John’s brain after his stroke (Case 1).
When he writes letters to friends, John often squeezes the text over to the right side of the page. An example of his writing performance is shown in Fig. 1.3. When dialling a telephone number that had been written down by a friend, John is surprised and frustrated by the frequency of the wrong numbers he gets. Although John can be made aware of his neglect in this and other situations, he nevertheless continues to make similar errors and often attempts to explain his problems in terms of others forgetting or equipment that does not work. Recently, he was particularly upset to find out that on several occasions over the previous week, he had totally ignored his two favourite grandchildren; they had been playing on the floor 6–8 feet away from him—on his left side!
John announces he is going to the toilet, but as he tries to back his wheelchair out from the table there is a loud metallic noise. He looks down to his right while repeatedly pushing the chair out with his leg. The obstruction is on the left side of his wheelchair. When this is pointed out to him by a nurse, he slowly looks over to his left and discovers the problem for the first time. Only then does he manage to extract himself and proceed through the ward towards the toilet. A few minutes later, there is a series of minor accidents as John collides his wheelchair into a door-post, a cabinet, and a fellow patient’s wheelchair, all located on his left side. Furthermore, having taken only right turns on the way to the toilet, John now finds himself totally lost. With some difficulty, he is directed to the toilet.
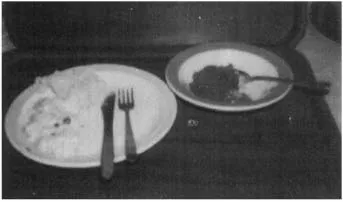
FIG. 1.2 Food neglected on the left side of plate.
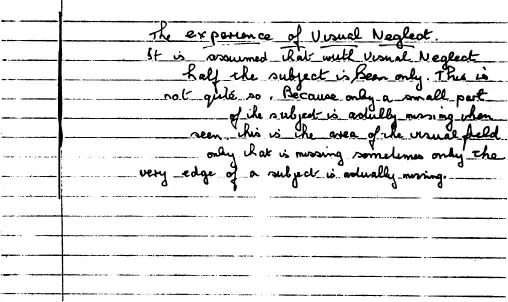
FIG. 1.3 An illustration of neglect dysgraphia: Writing is squeezed over to the right side of the page. Reproduced with permission from Halligan, P.W., and Robertson, I. (1992). The assessment of unilateral neglect. In J.R. Crawford, D.M. Parker & W.W. McKinlay (Eds.), A handbook of neuropsychological assessment (p. 159). Hove, UK: Lawrence Erlbaum Associates Ltd.
Another noticeable aspect of John’s behaviour is that he is prone to lapses of attention; his concentration appears to “drift off” during a task. This happens particularly in therapy sessions, where he has to be constantly reminded to attend to the exercises or tasks he is doing. His relatives also notice that he has difficulty following conversations when they are talking to him or when he is watching television.
Case 2: Rachel
Clinical presentation. Rachel is a 59-year-old school teacher who suffered a stroke three weeks previously. She suffered a large middle cerebral artery stroke, resulting in a mild left paralysis affecting her leg more than her arm. She has some sensation in her left arm, but shows marked sensory extinction (i.e. poor detection of left stimuli in the presence of right stimuli) when tested on double simultaneous stimulation. Her visual fields were full to confrontation testing. However, she also shows visual extinction when bilateral objects are presented simultaneously in her visual fields.
Behavioural observations. Most of the time, Rachel’s eyes and head are turned to her right-hand side; she appears unable to relax her neck muscles to allow her head to flex towards the hemiplegic side. Seated in her wheelchair, Rachel adopts a posture where her trunk is flexed; her head is turned to the right and most of the activities she engages in are located on her right side. When she co...
Table of contents
- Cover
- Half Title
- Title Page
- Copyright Page
- Table of Contents
- Acknowledgements
- Series preface
- 1. Clinical presentation of spatial neglect
- 2. Clinical issues for the diagnosis and interpretation of neglect
- 3. Assessment of visual neglect
- 4. Further assessments of neglect and related disorders
- 5. Recovery, variability, and early attempts to treat visual neglect
- 6. Different attempts to treat visual neglect
- References
- Author Index
- Subject Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Spatial Neglect by Peter W. Halligan,Ian Robertson,Peter W Halligan in PDF and/or ePUB format, as well as other popular books in Psychology & Cognitive Neuroscience & Neuropsychology. We have over 1.5 million books available in our catalogue for you to explore.