![]()
Part I
The brain and how it may be damaged
In the following chapters we provide some brief background information regarding the brain, its functioning and development as a basis to assist you further to understand, firstly the deficits that can be provoked by acquired brain injuries, and then the ways that we recommend that these can best be addressed when planning educational programmes for people with this condition.
The fact is that most of us have a general understanding of the effects of other types of injuries that are visible and of the parts of the body that these may affect. However, we often take for granted the most important organ in our bodies: our brain. We do not pause to think how this may function or how it may be injured. The effects of such injuries are so often misunderstood or misinterpreted.
The actress Jane Lapotaire, who sustained an acquired brain injury (ABI) in 2000, stated in an interview for the Telegraph in December 2014: ‘That’s the problem with brain injuries – you look the same, but everything’s changed. I have a long scar from here to there,’ she says, running her hand six inches along her skull to her right ear. ‘But no one can see it, so no one makes allowances for me.’
In her book, Time Out of Mind, published in 2003, she noted: ‘The hardest thing of all which made my sense of injustice boil and rage, was being judged on behaviour for which I was not responsible, over which I had no control.’
On 20 July 2010, James Cracknell, an Olympic Gold Medalist for rowing, sustained an ABI when he was hit from behind by a petrol tanker whilst cycling.
In an article published in the Telegraph newspaper in October 2012, Cracknell wrote, ‘Certainly I looked the same in the mirror, but I no longer knew if I was the same person. I had no consistent memory of the six weeks that followed the accident. I had to relearn most tasks and physical skills, even walking. To those around me, I was short-tempered, frustrated and angry.’
We hope to provide you with a glimpse of the brain and brain injuries in order that you can then have greater understanding, make allowances and not misjudge.
![]()
1
Brain Anatomy and Functions
The description of the brain and its functions within this chapter is intended to assist those who are not specialists in neurology towards a very basic understanding of the way that our brains function and the various components of this amazing organ. With even a superficial knowledge of brain functions, we can begin to predict the possible effects of a brain injury for an individual and also to understand the repercussions that may be manifest during future years.
For those wishing to acquire more detailed or scientifically based information regarding brain anatomy and neuro-cognitive functioning, there is a wealth of publications dedicated to these topics (e.g. Andrews (2009), Gazzaniga et al. (2009), Kolb and Whishaw (2009)). This section is intended to provide an accessible but introductory guide to readers for whom this is a relatively new topic.
Parts of the brain
The central nervous system is made up of the brain and the spinal cord, which acts as a connecting pathway through which the brain can relay information to and from all other parts of the body. Damage to the spinal cord (‘spinal injury’) is also neurological in nature but obviously provokes very different issues from damage to the brain, so is not included in the umbrella term of acquired brain injury (ABI).
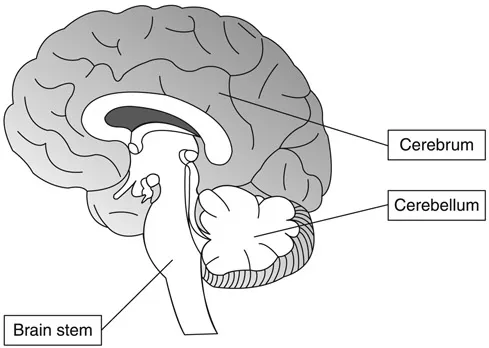
The brain basically comprises three major parts: the brainstem, the cerebellum and the cerebrum. Below are simple descriptions of the specific functions of each of these parts, but it must be remembered that none of these operate in isolation and the whole brain system of interconnected and inter-dependent neural connections is very complex.
The brainstem is at the base of the brain and connects with the top of the spinal cord. It is responsible for basic functions essential to life, such as breathing, heart rate and blood pressure, and it plays a vital role in basic arousal and consciousness. It is also involved with functions relating, for instance, to sleep patterns, hunger/thirst and swallowing. It is a focus for most cranial nerves, for instance those controlling movement and sensation within the face and mouth.
Figure 1.1 Cross-section of the brain
The cerebellum is found just above the brain stem and beneath the back of the cerebral cortex. This brain region is primarily responsible for the control and co-ordination of bodily movement and muscle tone. It is also important to our ability to learn and refine ‘patterns’ of movement (motor learning) used both in activities of daily living and selected physical or leisure skills. It may also be involved with some slightly more sophisticated cognitive functions.
The cerebrum is the largest part of the human brain, the outer layers of which are made up of: the cerebral cortex (a layer of grey matter); an underlying layer of white matter; and some important sub-cortical brain structures which are enveloped by the outer cortex.
The cerebral cortex is only found in mammals and is responsible for the most sophisticated levels of thought, movement and behaviour. It is divided into two halves – the right and left hemispheres. Although these two areas may appear as ‘mirror images’, they have different functions. The left cerebral hemisphere controls the physical and sensory functions of the right side of the body and is usually responsible for many speech and language functions; the right cerebral hemisphere controls the left side of the body and is usually responsible for many functions relating to visual, spatial and other non-verbal skills.
The two hemispheres are linked by a structure called the corpus callosum by which information is exchanged between the hemispheres.
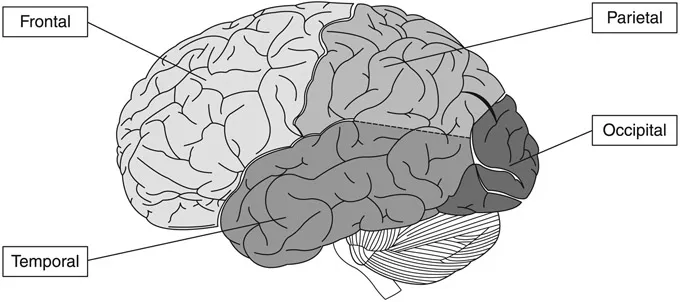
Each hemisphere of the cortex is comprised of four parts or lobes: occipital, parietal, temporal and frontal. Although, once again, this is a simplistic overview, each of these lobes is associated with different aspects of functioning:
Figure 1.2 Lobes of the cortex
The occipital lobes are at the lower part of the back of each hemisphere and are the visual processing centres of the brain. This includes rapidly making sense of the visual information registered by the eyes, processing visual signals and contributing to the awareness of visuo-spatial information.
The parietal lobes are situated at the back and top of the head, above the occipital lobes and the temporal lobes and behind the frontal lobes. They are responsible for the processing of information about body sensation, most particularly with regard to touch and other sensory inputs via our skin, such as pressure, temperature and pain. The parietal lobes are also concerned with integrating sensory information and visuo-spatial processing.
The temporal lobes are situated underneath the parietal lobes and underneath and behind the frontal lobes (behind the ears). They are important for processing auditory information and are highly associated with memory skills. They are also involved with many other processes, such as selective attention, musical ability, visual recognition (e.g. of faces) and aspects of language. An important area of the brain (named Wernicke’s area after the person who identified it) spans part of the temporal and parietal lobes and is responsible for much of our understanding (and production) of meaningful language.
The frontal lobes are located behind the forehead and are extremely vulnerable to injury because of this location at the front of the head. The inner surface of the skull is quite rough with bony ridges on the inside of the forehead so these also add to the vulnerability of frontal areas of the brain if they collide with the skull. This area is one of the most common regions of traumatic brain injury (Levin et al., 1987).
The frontal lobes contain another important language area, Broca’s area (also after the person who identified it), which is mainly associated with speech production although it is now known that it is also involved with some aspects of language comprehension (Caplan, 2006). These lobes are also responsible for some motor functions, in addition to factors affecting memory, but are often known mainly for their influence over emotional control and personality. They are very important with regard to problem solving, initiation, judgement, impulse control, social and sexual issues, and generally for the organisation, planning, evaluation and modulation of behaviour. Much of this is linked with what are termed ‘executive functions’ and these are very important when considering ABI. For further information see Chapter 7.
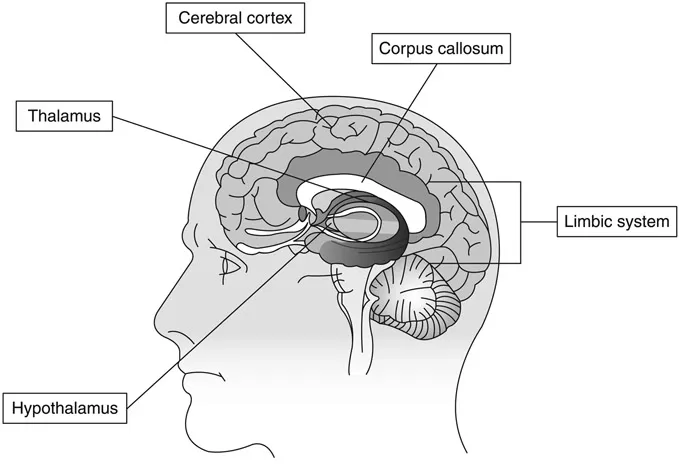
Other sub-cortical structures, such as those within the limbic system, the thalamus and the hypothalamus, are situated below the cerebral cortex. These have very important functions relating, for instance, to emotions (fear, aggression, happiness, pleasure etc.); to memory formation; to sleep and wakefulness; and to relaying sensory information.
In addition to the protection by the skull, the brain is also surrounded by three layers of membrane, which are known collectively as the meninges. The outer one is like a very tough plastic sheet and provides the brain with some protection, particularly during movement.
Under this, a clear watery-like liquid called cerebro-spinal fluid surrounds and cushions the brain. This is produced in four chambers, or ‘spaces’, within the brain called ventricles. The fluid flows through these and around the brain and spinal column.
Figure 1.3 Position of sub-cortical structures
There is also, of course, a blood supply to the brain, which provides oxygen and nutrients and removes waste products. A blood–brain barrier also filters the blood and provides some protection to the brain from any chemicals that could be toxic.
How does the brain function?
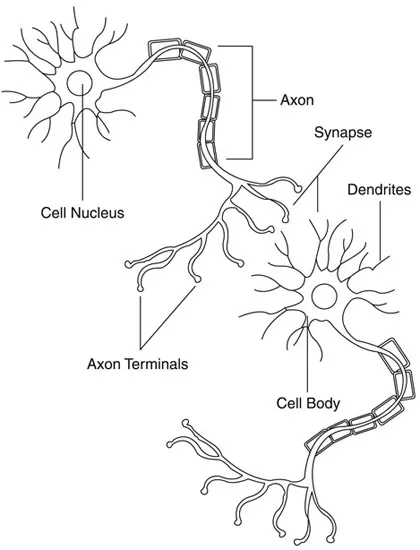
Figure 1.4 Neural connections
Brain tissue comprises cells called neurons which are among other cells called glial cells. Put simply, glial cells provide support and protection for the neurons and are involved in the production of an important substance called myelin, which is described later in this section. There are different types of specialist neurons but they are all able to transmit information through electrical and chemical signals and, therefore, to connect together to form what are termed neural networks. This communication occurs via microscopic fibres that grow attached to neurons. Some of these are called dendrites and each neuron may have many dendrites, which can also form branches. These are the fibres that receive messages to the neuron. Each neuron can have just one fibre that transmits messages (an axon), although each of these may also have multiple ‘branches’. The minute gaps by which messages are transmitted at the ends of these fibres are called synapses.
These neural networks develop as children mature but can also be formed, or discarded if no longer required, during adulthood. We have all heard reports of parts of the brains of certain individuals developing, such as taxi drivers who have to learn ‘visual maps’ and parts of their brains responsible for these skills being seen to have ‘grown’ on scans. This is not growth in terms of neurons, but an increase in the connections between them as these skills are used and practised. Conversely, if certain skills are never used, the connections responsible for enabling these can reduce or disappear.
The development from baby to adult in terms of neuro-cognition is also primarily a process of the establishment of new neural pathways and connections. Initially, these are relatively fragile but they then become more robust over time and with use: a ‘sheath’ of a substance called myelin gradually forms around axons to insulate them and to increase the speed at which messages can be conveyed. During development, these pathways can also be removed, or ‘pruned’ if not required. The initial time of neuro-cognitive development that occurs during childhood continues up until approximately 25 years of age. There are implications in terms of the potential effects on an ABI, depending on the developmental stage at which it occurred (see Chapter 3).
![]()
2
Acquired Brain Injury (ABI)
The definition of an acquired brain injury (ABI) is: an injury occurring to the brain after the first few weeks of life. Injuries to the brains of babies prior to birth or during that very early stage can provoke issues which have similarities to those seen in ABI, but the overall pattern and prognosis usually differs. The term also refers to injury provoked by a specific ‘event’, so degenerative conditions are not included. However, particularly in the ageing population, certain degenerative neuro-cognitive conditions can serve to exacerbate and complicate the effects of an ABI. There is also research to indicate that some people who have sustained an ABI may be more at risk for developing other neurological conditions later in life (Bazarian et al., 2009)
ABI may be caused by accidents or by diseases or infections. It is an ‘umbrella’ term, referring to what can be sub-divided as:
- traumatic brain injury (TBI) – caused by external forces, i.e. accidents or other injuries (sometimes previously termed a ‘head injury’)
- atraumatic or non-traumatic brain injury – caused by illness or infection affecting the brain.
Traumatic brain injury (TBI)
Such an injury can be caused when an object enters a specific area of the brain through the skull, such as in knife or gunshot wounds. These are termed penetrating brain injuries and, as the exact and often limited location of the injury can be seen, it may then be easier to predict the potential effects of this for the individual, with our knowledge of brain anatomy.
However, this occurs in a relatively small number of cases of TBI and, much more usually, the damage is more widespread. This can be in other cases where the skull has been damaged or in those where there is no skull fracture. Some of the most commonly seen of this latter group, most usually resulting from road traffic accidents, are termed: acceleration/deceleration injuries. These form part of a group termed closed brain injuries. Imagine travelling in a vehicle at speed and then coming to an abrupt stop on impact. This can cause the brain to be shaken violently and sometimes twisted from the pivotal point at its base. It may have collided with the front and back of the skull as the ‘cushioning’ of the meninges and cerebro-spinal fluid is insufficient to prevent this. This can cause the brain to bru...