![]()
Chapter 1
An introduction to brief group psychotherapy in intensive care programmes for eating disorders: gathering research evidence
Kate Tchanturia and Katherine Sparrow
Eating disorders are severe mental health problems with devastating consequences. The high mortality rates associated with these disorders emphasise the relevance of developing successful treatment interventions. The existing literature regarding psychological treatment programmes for eating disorders is still limited, and this is particularly true for group interventions.
Delivering psychological interventions in a group format can bring unique benefits that are not achievable when working with patients individually. These benefits include: sharing experiences and learning from others in a safe and therapeutic environment, being with other people and practising interpersonal skills. In the treatment of anorexia nervosa (AN), these therapeutic benefits also represent a challenge for group facilitators as it is exactly these interpersonal and relational demands that patients find difficult to tolerate (Tchanturia et al., 2012, 2013a; Fleming et al., 2014). Facilitators are likely to be confronted with low motivation and a reluctance to engage, which are not only characteristic of the illness itself, but are also a result of the discomfort evoked by spending time with others in a group setting (Genders and Tchanturia, 2010). It has been observed that patients with AN often remain isolated and avoid communicating with other patients in inpatient settings. Our recent research also shows that people with anorexia have difficulties making social contacts and forming friendships well before the onset of the illness (Doris et al., 2014). We also know that people with eating disorders report high levels of social anhedonia – an absence of pleasure derived from being with people (Tchanturia et al., 2012; Harrison et al., 2014). In our recent study when we compared IQ matched controls and patients with anorexia, we found that patients with a higher than normal IQ scored lower on emotional intelligence tasks (Hambrook et al., 2012). This task called MSCIT is widely used in human resources and by organisational psychologists. A combination of many factors such as being shy, socially anxious and having a long-term eating disorder creates social difficulties. The majority of patients in our inpatient programme tell us about their discomfort when engaging in group discussions, whether inside or outside of the hospital environment. In one of our recent studies exploring how eating disorders affect work and social adjustment we found that most people experienced the largest detriment to their social relationships and social leisure, whereas the work domain was less affected by their eating disorder (Tchanturia et al., 2013a; Harrison et al., 2014). One interesting piece of research conducted by our group suggests that patients with anorexia have very low facial expressivity in the acute stage of the illness. While watching an amusing film clip, patients with anorexia did not express smiles compared to non-eating-disordered controls (Davies et al., 2010). Interestingly, the results of this original study conducted with adults were replicated in an adolescent patient group (Rhind et al., 2014). The absence of facial emotional expression hugely affects the quality of patients’ relationships. We have therefore used these research findings to inform our group interventions and tailor group treatment in the best possible way for our patients. For example, we developed psychoeducation materials and specific exercises informed by research findings to help patients address their social difficulties.
Group therapy is unique in providing a safe opportunity to address social problems, which is important for improving patients’ quality of life and relapse prevention. For this reason we have summarised the relevant literature in this book to enable us to reflect on our own practice and develop a stronger, more robust group treatment programme.
We utilise a stringent clinical audit system in our treatment programme in order to evaluate the efficacy of both individual and group interventions. Over the years we have been considering how to improve the group programme and tailor it to our patients’ needs. This is an ongoing process and we have shared our insights in this book with the aim to help both ourselves and our colleagues working in the field of eating disorders to learn from this research and develop group treatment programmes further.
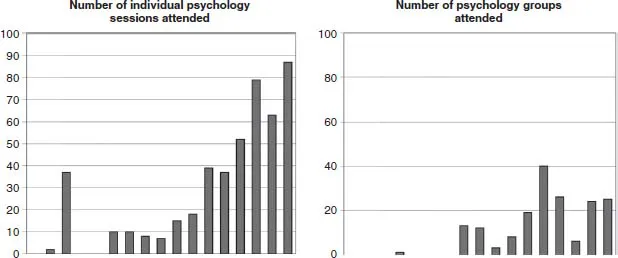
In Figure 1.1 we have presented a brief snapshot of the number of individual vs group therapy sessions attended by inpatients on our ward in 2013. This provides a visual demonstration of the challenges faced by clinicians regarding patients’ willingness to engage with group treatment. On examination of the individual cases presented in Figure 1.1, it appears that patients who attended a relatively greater number of individual therapy sessions are those who failed to gain significant weight during their inpatient admission and remained on the ward for a long time. It is notable that the number of group therapy sessions attended by these patients is very low.
In contrast, patients who attended relatively fewer individual therapy sessions and a relatively greater number of group therapy sessions were more likely to gain weight and have a shorter admission period. These observations are very preliminary and complex, but nevertheless emphasise the importance of encouraging patients to attend group therapy. This approach holds great therapeutic value for patients. The group format encourages them to be with others and to develop the skills to eat in a social environment. Patients also have the opportunity to discuss topics directly related to the disorder or to broader aspects of recovery. In addition, given the busy ward environment, a meaningful and evidence-based group programme is a more efficient use of the therapist’s time; a necessary consideration which will be further explained later.
Figure 1.1 Snapshot of the individual and group attendance
Having highlighted these difficulties, we believe it would be therapeutically beneficial to use the time during an inpatient’s admission to address not only the core symptoms of the illness, but also the broader issues which often act as maintaining factors. Therapeutic interventions which improve interpersonal skills and confidence in being with others, and create a more cohesive sense of identity and reduce feelings of isolation, are likely to facilitate the complex process of functional reintegration into the community. Some authors believe that interventions which encourage the direct expression of feelings are clearly warranted in this patient group, as they are inclined to express feelings through indirect or somatic channels (Lieb and Thompson, 1984). Therapeutic groups are the ideal place to practise and implement social and communication skills, and to receive social feedback (both verbal and non-verbal). In the context of inpatient adult services, the majority of patients have a chronic eating disorder and have been unwell for many years (Chapter 3 has more specific information about our national clinic demographics), therefore their social network is limited and their social confidence is low. To add to these difficulties, the prevalence of autistic traits is high among eating disordered inpatients (e.g. Huke et al., 2013; Tchanturia et al., 2013c).
There has been a great deal of research and clinical debate regarding what works best in terms of treatment for eating disorders in adults. This is particularly true for patients with a diagnosis of anorexia due to the lack of a strong first choice treatment (NICE, 2004). Another problematic issue related to this is that it tends to be the more severely unwell patients who disengage from treatment. Given that AN has a high mortality rate and is a huge burden for patients, their families and society, further research and new recommendations are needed.
With regard to the existing literature for group interventions, the majority of recently published studies focus only on individual forms of treatment. Indeed, our systematic appraisal of the literature showed that only 38 studies have reported group therapy treatments in eating disorders. Moreover it is difficult to form any conclusions from the available studies for the following reasons: they report on different patient groups (anorexia, bulimia, binge eating disorders), the content and therapeutic model varies hugely, sample sizes are small, and outcome measures are very different (Genders and Tchanturia, 2010; Pretorius et al., 2012; Fleming et al., 2014).
We decided to appraise the available literature and present the studies we were able to find systematically before publishing this book. Table 1.1 summarises the studies we were able to find up to and including 2014 (May).
Systematic literature review of the group treatment of EDs: method
Two systematic literature reviews were conducted according to the ‘PRISMA statement’ (Moher...