![]()
Chapter 1
Introduction to clinical exercise science
Andrew Scott
Introduction
This book has been developed to complement other similar books in the area of clinical exercise science by bringing together expert exercise practitioners in the UK who also have an academic background, to provide evidence-based exercise guidance that academic texts in clinical exercise do not provide. This textbook aims to discuss information on exercise considerations for medical conditions in Chapters 2–10, and also discusses methods of facilitating exercise referral and long-term physical activity behaviour change in Chapters 11–14.
This chapter and the subsequent chapters in the book follow a general pattern including:
• A brief discussion of the pathophysiology of the condition
• Specific exercise guidelines and a discussion of the evidence that underpins these
• A case study
• Suggestions for future research
• A chapter summary
• Study tasks
• Further reading/resources.
A key theme in this book is the promotion of physical activity, not just the study of exercise physiology, as is the case with many such textbooks and, especially, journal articles. There is often a disconnection between working in an ideal physiological scenario, yet forgetting that those who can benefit from being more physically active will not necessarily have the contacts, intrinsic motivation, or confidence to become more physically active by themselves. Therefore, the remit of this book was to bring together a team of authors who are not only exercise scientists, but are also experienced practitioners in the study of physical activity, and are themselves exercise practitioners. This has led to a practitioner focus to the chapters rather than them just reporting data from laboratory studies. Importantly, there are four chapters that are focused on the soft skills of engaging sedentary individuals in becoming more physically active using evidence-based research and the professional experiences of the authors.
Chapters 2–9 in this book are largely defined by the range of specialist exercise instructor awards for the management of chronic diseases or disorders that are available in the UK, while Chapter 10 presents information on well-established techniques being applied in a relatively new context that have not been presented in other such textbooks. Exercise services in cardiac rehabilitation, pulmonary rehabilitation, stroke rehabilitation, neurological rehabilitation, and physiotherapy for musculoskeletal conditions are well-established in hospitals in the UK; however, referral pathways for patients following outpatient care can be variable. Referral for exercise for individuals recovering from cancer treatment is increasing, although it is still not widely available, while dedicated physical activity counselling for diabetes and mental health needs to be prioritised in care pathways, since increasing numbers of patients are suffering from such disorders, which have a strong and inverse relationship with physical activity and fitness levels. Chapter 10 is not related to exercise leadership per se, but is concerned with the increasing utilisation of pre-operative exercise testing to objectively assess a patient’s fitness for surgery rather than clinical judgement alone. Such tests can be used to indicate to a patient how much they might struggle during the peri-operative period (during and after surgery). In previous years, these tests would screen out patients who would be unable to receive surgical treatment – usually for cancer resection – however, increasing research has demonstrated that, as with apparently healthy individuals, it is possible to significantly and clinically improve fitness for surgery through structured exercise training. The remaining challenge is to optimise the exercise prescription for improving fitness for surgery and post-surgical prognosis with the minimum of frequency, intensity, and time of exercise.
The final four chapters in the book present the authors’ experience of promoting health behaviours in a physical activity context, particularly relating to exercise referral services in the UK. The use of physical activity counselling underpinned by psychological principles is under-utilised in the UK, with behavioural medicine still not as available as traditional medicine in the prevention and treatment of chronic diseases and disorders. This is further exacerbated by sport and exercise psychology, and, indeed, often sport and exercise in general, being largely focused on sport and less on exercise. There is often a token nod to physical activity in most respects, rather than the promotion of health-enhancing physical activity being the primary focus that is needed to help the National Health Service (NHS) and regional and central governments in their challenge to engage individuals in physical activity across the lifespan of diverse groups of individuals. Chapter 11 outlines the theory and application of psychological principles to enhancing health behaviours and parallels this with physical activity, where there is less evidence. Chapters 12 and 13 discuss the promotion of physical activity through an evaluation of research interventions, and those applied specifically in exercise referral services. Finally, Chapter 14 discusses the relatively new advent of ‘stealth physical activity interventions’ to enhance physical activity participation in hard-to-reach groups, i.e. those who do not wish to take part in structured physical activity or do not personally take responsibility for their health. The message is to perform a particular activity, such as gardening, as the primary driver to deliver an end result, i.e. a tidy garden, but at the same time increase incidental energy expenditure too.
Physical activity in healthcare
During the last fifty years there has been considerable growth in the appreciation of physical activity in preventive medicine and in the secondary treatment of a range of communicable and non-communicable disorders, based on a range of anecdotal, epidemiological, and interventional reports (Blair and Morris, 2009; Fiuza-Luces et al., 2013; Sallis, 2009). The evidence is so broad that physical inactivity is increasingly being seen as a key public health issue, equal to smoking and obesity (Kohl et al., 2012; Lee et al., 2012). In the general population, it has long been recognised that engaging adults in regular exercise could achieve important health benefits at relatively low cost (Morris, 1994). Physical activity reduces the risk of developing chronic diseases including type 2 diabetes (Hopper et al., 2011), cancer of the breast (Friedenreich, 2011), kidney (Behrens and Leitzmann, 2013) and colon (Thompson et al., 2003), osteoporosis (Howe et al., 2011), obesity (Tate et al., 2007) and depression (Mammen and Faulkner, 2013). Further benefits may include increased employment rates and decreased mental health problems for both patients and carers.
Fitter patients have been shown to have better outcomes in a wide variety of conditions, including diabetes (Hayashino et al., 2012; Thomas et al., 2006), coronary artery disease (Thompson et al., 2003; Thompson et al., 2007), heart failure (Belardinelli et al., 1999; Mandic et al., 2012; O’Connor et al., 2009), hypertension (Cornelissen and Smart, 2013), COPD (Waschki et al., 2011), chronic kidney disease (Heiwe and Jacobson, 2011), cancer (Brunelli et al. 2014; Des Guetz et al., 2013), stroke (Austin et al., 2014; Saunders et al., 2013), depression (Cooney et al., 2013) and dementia (Forbes et al., 2013).
Although there is a transiently-increased risk of mortality during physical activity or training (De Backer et al., 2003; Thompson et al., 2007), this is outweighed by the cumulative benefit of regular physical activity (Thompson et al., 2003). Supervised and unsupervised training programmes have been shown to be beneficial in a variety of conditions, including COPD, stroke, heart failure, and intermittent claudication (Carson et al., 2013; Lane et al., 2014; Mehrholz et al., 2014; Puhan et al., 2011; Taylor et al., 2014). Furthermore, exercise has been shown to improve the quality of life and the ability to perform activities of daily living in the frail elderly (Chou et al., 2012). Likewise, the public health promotion of physical activity is generally effective (Heath et al., 2012).
Exercise referral services
The evidence for physical activity in the management of long-term health conditions is now beginning to be implemented through the development of condition-specific community exercise programmes in the UK. The referral pathways for various medical conditions are analogous to the well-established rehabilitation services for patients with cardiac disease, where patients graduate from outpatient rehabilitation programmes and are referred to community-based exercise programmes that are sometimes part of broader exercise referral services. These collaborations between NHS Trusts and council-run leisure centres provide a range of exercise programmes delivered in either small group or one-to-one sessions (Nicholson et al., 2013). Additionally, some UK charities, such as Breathe Easy, Action from Rehabilitation for Neurological Injury (ARNI), MacMillan and Mind offer free or minimal-cost group exercise classes.
As with all health interventions the cost-effectiveness of exercise referral has been scrutinised. The available evidence suggests that structured exercise is one of the most cost-effective interventions available, using chronic obstructive pulmonary disease (COPD) as an example. A recent summary of the relative value of treatments for COPD suggested that pulmonary rehabilitation (PR) was one of the highest value interventions to improve health outcomes in this patient group (British Thoracic Society, 2012). However, even in the optimal environment of an outpatient unit, the time dedicated to each patient’s therapy is restricted by economic constraints, such as limited resources and personnel (Gallanagh et al., 2011). Individual therapy is labour intensive (Studenski et al. 2005), whereas reduced self-esteem and low mood in patients can contribute to decreased motivation to participate in group-based physical activity (Gallanagh et al., 2011). However, circuit class therapy (CCT) can be as effective as individual physiotherapy sessions for inpatient rehabilitation and in reducing the length of hospital stay (English and Hillier, 2011; English et al., 2007). Thus, the provision of CCT over individual therapy is more cost-effective, and also facilitates socialisation and the reduction of perceptions of isolation. An age-old yet persistent challenge is increasing the ‘graduation’ of patients receiving acute hospital-based exercise therapy, such as cardiac rehabilitation, pulmonary rehabilitation, stroke rehabilitation or cancer treatment, into community-based physical activity programmes to maintain lifelong physical activity to help in secondary prevention. The main challenge here, besides funding, is ensuring that exercise practitioners engage in appropriate training, gain experience, and maintain their continuing professional development in planning, instructing, and adapting physical activities for a range of referred conditions. This is important since such individuals are increasingly presenting with multiple morbidities besides their primary referral condition.
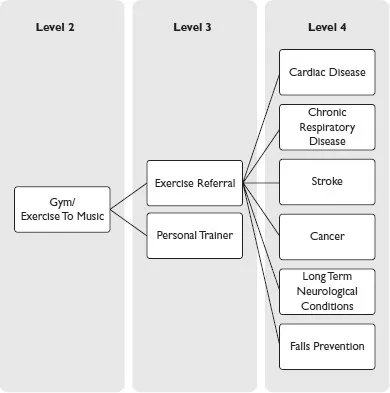
Physical activity and health training pathways
Professionals involved in the delivery of hospital- and community-based clinical exercise services require condition-specific training and experience in prescribing and supervising exercise for such patient groups, along with up to date cardiopulmonary resuscitation (CPR) training. Referral pathways may include input from professionals in several disciplines, including: general physicians, consultants, physiotherapists, occupational therapists, nurses, dieticians, exercise physiologists, and health psychologists. The balance of the contribution of these healthcare professionals depends on the particular patient group and the level of service that has been commissioned. A number of training pathways are available for individuals to train to deliver clinical exercise programmes, and those in the UK and USA will be discussed here.
UK accredited certifications