A second edition of a text that demonstrates how personnel management can contribute to general practice. Case studies and examples are used throughout.
Learning without thought is labour lost; thought without learning is perilous.
Confucius (c.550-c478 BC)
Who should read this chapter?
There are three reasons why you should read this chapter:
You don’t have any form of an electronic patient record (EPR) system at the moment and require convincing that the hassle and expense are worth the benefits to be gained.
You have an EPR system but it is ineffectual and out of date and you need reminding as to why it seemed such a good idea at the time, before committing yourself to repeating that hassle and expense by changing your system.
You are simply reading this book from beginning to end in an effort to cure insomnia. Personally, I’d recommend a warm bath and a hot milky drink.
Once upon a time ...
... there was a young GP, Dr Jones. Dr Jones had recently become a partner at the ABC Health Centre in British Columbia. The primary care team at the ABC Health Centre consists of a nurse practitioner, a practice nurse, two medical office assistants (MOA), an office manager, Dr Thomas, Dr Andrews and of course Dr Jones. Several other health practitioners also share their premises. Dr Jones’ partners have little time for technology and whilst they do have an electronic patient record system, they make very little use of it.
Dr Jones is frustrated by the practice’s use of paper records. Whilst a GP resident and medical student he worked in several practices that used electronic patient records and feels that there is a lot of benefit that their practice could gain from their use.
Although he is happy to take on the management of information communication technologies (ICT) within the practice he recognizes that first he needs to convince his partners that there are benefits from using an EPR system more effectively. However, he also knows that the system the practice currently has is very outdated and that considerable time and money may be required before these benefits can be gained.
During the weekly primary care team meeting he asks his colleagues what they think of their current EPR system. He is not surprised to find that they consider it useless and antiquated. After some discussion, he suggests that at the next team meeting they set aside some time to discuss this further.
This may or may not be a fairy story. However, it is true that there are many practices that either do not have an electronic patient record system or make little use of what they have. Therefore, let us consider Dr Jones for a moment. At his next primary care team meeting, his general practitioner (GP) colleagues will undoubtedly air a long list of complaints about their current system. They will quote the amount of money it cost to purchase and to maintain. They will be emphatic that patients do not wish them to use it.
The electronic patient record - why?
So how will Dr Jones persuade his colleagues that investing in their EPR is a good idea? Let’s look at the evidence.
Managing and providing primary care-based patient care would be a simple prospect if patients:
have just one medical condition
never have medical emergencies
never require secondary or tertiary care
never travel beyond their home town
never see more than one healthcare provider.
Unfortunately, this is not the case. Consequently, what has developed in primary care is the cradle-to-grave (or sperm-to-worm) record. This ‘record’ documents all ailments, treatments and interventions, allowing each person reading that record to know what has gone before.
Historically, this ‘document’ has been paper-based and has followed a patient around the country each time they start regularly attending a new general practice. However, since the mid-1970s more and more GPs, internationally, have opted to keep this record, to a greater or lesser extent, electronically. Why?
The carrot and stick
There are two reasons why GPs have opted to use EPR systems. The first is the carrot - personal (or practice)-based benefits. The second is the stick (sometimes cunningly disguised as a carrot) - key reforms and Government-led incentives.
Dr Jones prepared well for the primary care team meeting. He agreed that their current EPR had cost a lot of money and that there were issues that needed to be addressed. However, he also identified all the benefits that he had experienced when he had used an EPR in a ‘paperless’ practice. During the discussion, the MOA staff said that they thought a computerized scheduling system would be wonderful. Dr Thomas and Dr Andrews agreed that when they thought about it, they had actually gained financially from their limited use of their EPR through better management of billing. Dr Thomas also observed that there were far less calls from pharmacists clarifying prescriptions since they had started printing the prescriptions.
Being a tactful doctor, Dr Jones didn’t suggest that the practice should consider going ‘paperless’ but instead suggested that he undertake a little research to find out what the practice needed, what was available and what the likely requirements were going to be on the practice from the local health authority (HA) and provincial ministry of health. The primary care team were now interested in the potential whilst remaining sceptical. Dr Jones agreed to speak with their local HA information communication technology (ICT) manager and to report back at the next meeting.
Appendix 1 provides a detailed and referenced list of benefits attributed to primary care EPRs.
Personal and practice-based benefits
Finance: Practice income depends to a large extent on how well its’ patient population is managed. Typically EPRs maintain patient registers sorted alphabetically, by age and sex for screening/recall, for chronic diseases, and for repeat prescriptions. These age/sex and chronic disease registers can be used to call patients for fee-paying procedures thus increasing uptake and consequential financial payment.
Prescribing: Computerized repeat prescribing has been proven to save a lot of time and effort, and in general electronic prescribing is believed to improve safety due to a combination of inbuilt contraindication alerts and the use of printed prescriptions as opposed to hand written, often illegible scripts.
Clinical governance: The number of areas where practices are mandated to maintain chronic disease registers, minimum data sets and to report on the process of care is increasing. The use of an EPR is ideally suited to meet these requirements.
Clinical decision support tools: The primary care team cannot be expected to know everything as the medical knowledge base is growing exponentially. The use of validated decision support tools, protocols, guidelines and templates can help to address this (e.g. drug interventions, healthcare mai...
Table of contents
Cover
Title Page
Copyright Page
Contents
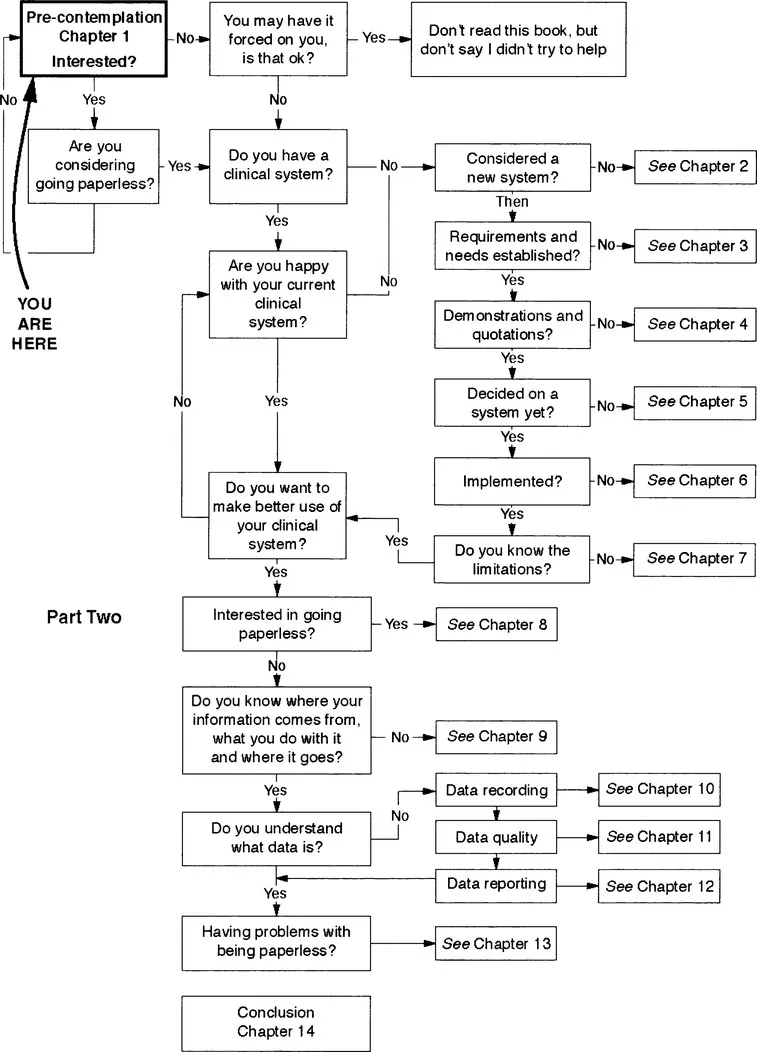
Contents map
Foreword
Preface
Acknowledgments
Part One: Choosing a clinical system
Part Two: Going paperless
Glossary
Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.4M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
Both plans are available with monthly, semester, or annual billing cycles.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go. Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Computerization and Going Paperless in Canadian Primary Care by Nicola Shaw in PDF and/or ePUB format, as well as other popular books in Medicine & Medical Theory, Practice & Reference. We have over one million books available in our catalogue for you to explore.