- 268 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
Thoracic Surgery: 50 Challenging cases
About this book
In Thoracic Surgery: 50 Challenging Cases, editor Wickii T. Vigneswaran has selected 50 challenging cases presented by leading thoracic surgeons. Each case highlights a unique situation from which other surgeons can learn. The selection of Cases includes patients with diagnostic challenges, unconventional and innovative solutions, unexpected findings, and new techniques to treat old problems. The discussions after each case provide a useful starting point for further inquiry. Amply illustrated, this book reflects the wisdom and experience of world leaders in thoracic surgery and teaches junior surgeons how to approach the key thoracic surgical procedures, and how to manage in unexpected and difficult situations. This is a Masterclass in thoracic surgery.
Editor Bio
Wickii T. Vigneswaran is the Professor and Chief of Thoracic Surgery for the Department of Thoracic and Cardiovascular Surgery at Loyola University Health System.
Tools to learn more effectively

Saving Books

Keyword Search

Annotating Text

Listen to it instead
Information
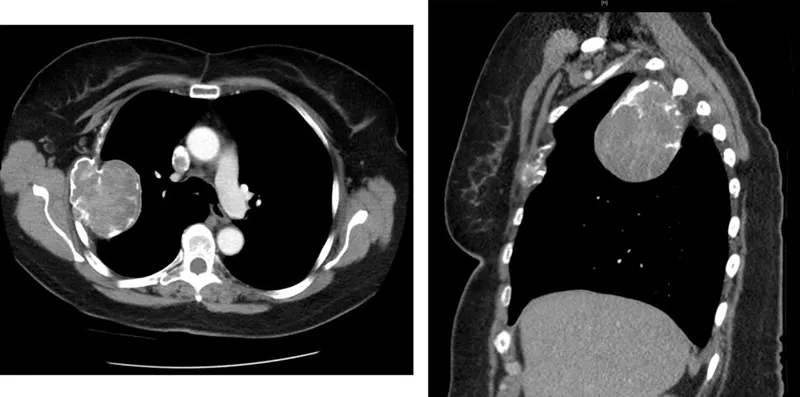
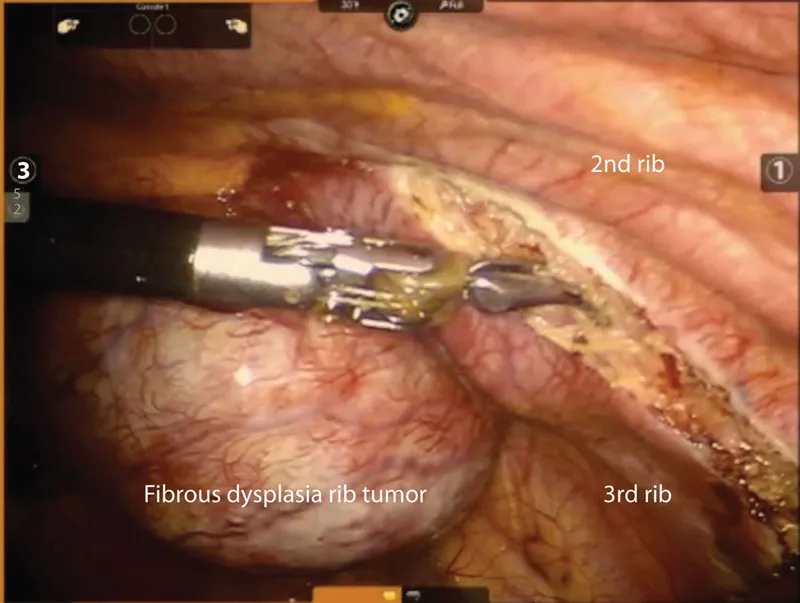
CASE 1: ROBOTIC-ASSISTED RESECTION OF FIBROUS DYSPLASIA OF THE RIBS
Hiroko Nakahama and Wickii T. Vigneswaran
 | Key Words |
| • Robotic-assisted thoracoscopic surgery • Fibrous dysplasia • Chest wall tumor | |
Introduction
Case Report
Comments
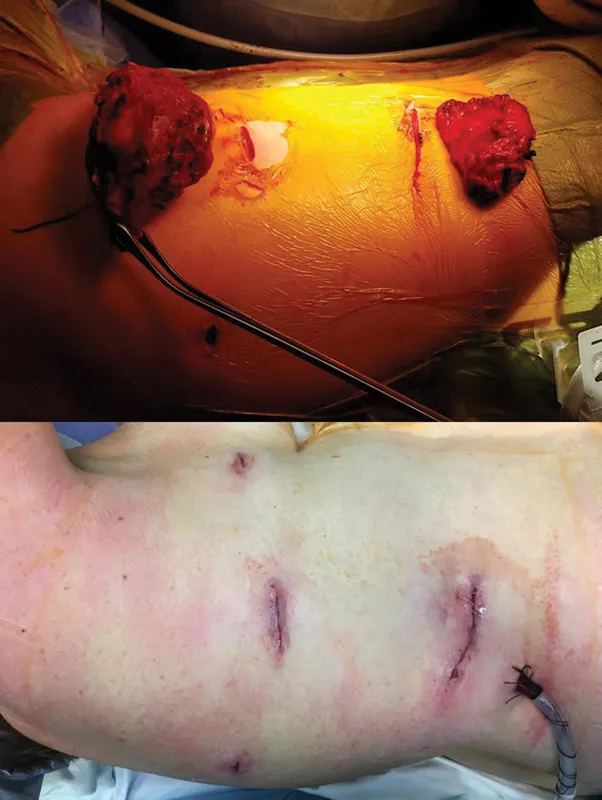
Table of contents
- Cover
- Half Title
- Title Page
- Copyright Page
- Dedication
- Table of Contents
- Preface
- Acknowledgments
- Editor
- Contributors
- Case 1: Robotic-Assisted Resection of Fibrous Dysplasia of the Ribs
- Case 2: Innovative Approach to Minimally Invasive Resection of a Second Rib Aneurysmal Bone Cyst
- Case 3: Hybrid Approach to Repair of Acquired Thoracic Dystrophy in an Adult Patient after Failed Childhood Ravitch Procedure
- Case 4: Cystic Bone Lesion of the Sternum
- Case 5: Spontaneous Bilateral Sternoclavicular Joint Infections
- Case 6: Malignant Solitary Fibrous Tumor of the Pleura
- Case 7: Malignant Solitary Fibrous Tumor of the Pleura with Chest Wall Invasion—Treated with Chest Wall Resection, Reconstruction, and Adjuvant Proton Beam Radiotherapy
- Case 8: Empyema from Misplacement of Percutaneous Nephrostomy Tube—A Diagnostic Challenge
- Case 9: Malignant Solitary Fibrous Tumor of the Pleura Associated with a Paraneoplastic Hypoglycemia
- Case 10: Feculent Empyema after Laparoscopic Appendectomy
- Case 11: Robotic Stapled Plication of a Left Hemidiaphragm Eventration
- Case 12: Iatrogenic Diaphragmatic Hernia Causing Total Right Lung Atelectasis
- Case 13: Successful Repair of Right Diaphragmatic Herniation with Recovery of Liver Function
- Case 14: Late Presentation of a Post-traumatic Diaphragmatic Hernia
- Case 15: Resection of a Giant Posterior Mediastinal Ganglioneuroma
- Case 16: An Unexpected Schwannoma of the Phrenic Nerve
- Case 17: Acute Life-threatening Mediastinal Complications of Histoplasmosis
- Case 18: Mediastinal Liposarcoma after Remote History of Radiation as an Infant
- Case 19: Pseudo-aneurysm of Descending Aorta Presenting as Incarcerated Intrathoracic Stomach
- Case 20: Tracheal Chondrosarcoma
- Case 21: Multi-technique Management of Persistent Postintubation Tracheoesophageal Fistula in a Patient with Achalasia
- Case 22: Presentation of a Congenital Tracheal-Esophageal Fistula in Adolescence
- Case 23: Repair of a Near Full-Length Malignant Tracheal-Esophageal Fistula—A 17-Year Success Story
- Case 24: Gastrobronchial Fistula and Central Diaphragmatic Hernia After Sleeve Gastrectomy
- Case 25: A Bronchogenic Cyst Masquerading as a Paraesophageal Hiatal Hernia
- Case 26: The Surgical Treatment of Pulmonary Echinococcosis
- Case 27: Unusual Case of an Flurodeoxyglucose (FDG)-avid Non-Malignant Solitary Lung Mass
- Case 28: Intralobar Pulmonary Sequestration with Aberrant Venous Drainage
- Case 29: Pulmonary Dogworm (Dirofilaria immitis) Infection Presenting as a Solitary Pulmonary Nodule
- Case 30: Concurrent Congenital Diaphragmatic Hernia and Extralobar Pulmonary Sequestration
- Case 31: Primary Colloid Carcinoma of Lung
- Case 32: Pulmonary Mucormycosis with a Staphylococcus epidermidis Co-infection
- Case 33: A Complicated Pulmonary Cystic Echinococcosis in Pregnancy
- Case 34: Staged Bilateral Uniportal Video-Assisted Thoracoscopic Surgery (U-VATS) Extended Lung Resection for Chronic Bronchiectasis
- Case 35: Robotic Lobectomy in a Patient with Bronchiectasis and Diffuse Pleural Adhesions—Advantages Over Challenges
- Case 36: Successful Pulmonary Rescue of Adult Onset Granulomatosis with Polyangiitis Using Extracorporeal Membrane Oxygenation and Window Thoracostomy
- Case 37: Intimal Sarcoma of the Pulmonary Artery
- Case 38: An Obstructing Benign Fibroepithelial Polyp
- Case 39: Getting the “Gist” of Esophageal Gastrointestinal Stromal Tumors (GISTs)
- Case 40: Acute Esophageal Necrosis in Prader–Willi Syndrome
- Case 41: Enucleation of a Giant Esophageal Leiomyoma with Primary Esophageal Repair
- Case 42: Primary Colon Cancer in an Interposition Graft Following Esophagectomy
- Case 43: Mixed Cavernous Hemangioma-Lymphangioma of the Gastroesophageal Junction
- Case 44: Aortoesophageal Fistula, a Complication of Esophageal Stent Placement
- Case 45: Managing an Unusual Case of a Long Segment Benign Esophageal Stricture
- Case 46: Post-esophagectomy Colon Diaphragmatic Herniation
- Case 47: Normalized Blood Gases and Improved Pulmonary Function after Lung Volume Reduction Surgery in a Patient with Severe Global Respiratory Insufficiency
- Case 48: Bilateral Lobar Lung Transplantation with Extra-corporal Life Support (ECLS) in a Jehovah’s Witness
- Case 49: Single-Lung Transplant Recipient with Primary Carcinoma Metastasis from Native Lung to Donor Lung Allograft
- Case 50: Multistage Approach to Lung Transplantation in a Cystic Fibrosis Patient with Chronic Superior Vena Cava Occlusion and Patent Foramen Ovale
- Index
Frequently asked questions
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.4M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app